
Urethral catheterisation is a routine task that is frequently performed within a healthcare setting. Almost 25% of hospitalised patients are catheterised during their inpatient stay.1 Urethral injury typically occurs in men when the catheter’s anchoring balloon is inadvertently inflated inside the urethra.2 Short-term complications include pain, bleeding, and acute urinary retention.2 Urethral rupture can lead to the long-term complication of urethral stricture disease and may require urethral reconstruction in severe cases.2
There are currently no studies that demonstrate urethral strain thresholds for rupture during traumatic urethral catheterisation. Our aim was to investigate internal urethral diametric strain and threshold maximum inflation pressure as parameters for urethral rupture during inadvertent inflation of a catheter anchoring balloon in the urethra. In addition, we also designed and evaluated a novel safety device with the inability to cause urethral trauma, despite inadvertent balloon inflation in the urethra based on these parameters.
Inflation of a urethral catheter anchoring balloon was performed in the bulbar urethra of 21 ex vivo porcine models using 16 Fr catheters. Urethral trauma was characterised and graded with retrograde urethrography. Urethral rupture was correlated with internal urethral diametric strain (%) and maximal urethral pressure threshold values in kilopascals (kPa). Internal urethral diametric strain was calculated by averaging urethra luminal diameter proximal and distal to the traumatised site, and maximum luminal diameter at the traumatised site. Urethral catheters were then inflated in the bulbar urethras of seven fresh male cadavers using a standard syringe and a prototype safety-syringe prototype safety-syringe (Figure 1). The plunger of the standard syringe was depressed until opposing resistance pressure generated by the urethra prevented further inflation of the anchoring balloon. The plunger of the prototype safety-syringe was depressed until sterile water in the syringe decanted through an activated safety threshold pressure valve (Figure 1).
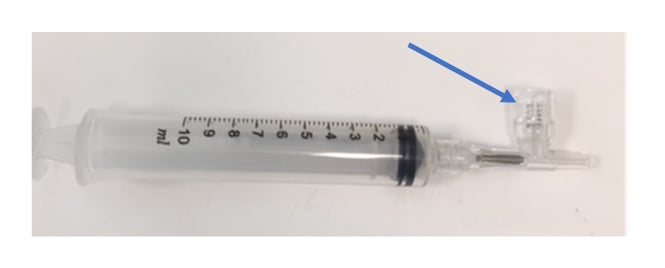
Figure 1: The prototype syringe used to determine urethral resistance pressure. The safety valve (arrow) is activated at threshold resistance pressure, allowing fluid to vent out of the activated valve.
Retrograde urethrography demonstrated that porcine urethral rupture consistently occurred at an internal urethral diametric strain >40% and a maximum inflation pressure >150 kPa (Figure 2). The mean±standard deviation maximum human urethral threshold inflation pressure required to activate the safety prototype syringe pressure valve was 153±3 kPa. In comparison, the mean maximum inflation pressure was significantly greater using the standard syringe than the activated prototype syringe (452±188 kPa, [p<0.001]).
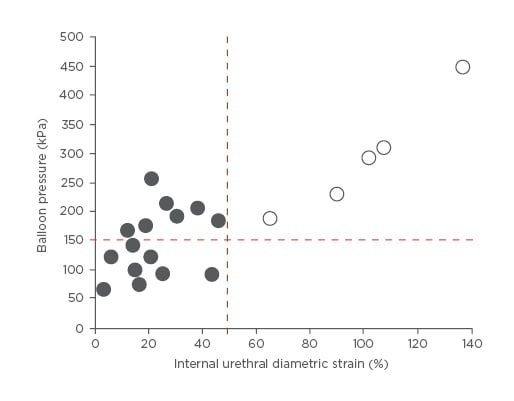
Figure 2: Maximum catheter balloon/urethral pressure and internal diametric strain recorded for each of the 21 urethral samples tested.
This figure clearly demonstrates a safety cut-off of >40% internal urethral diametric strain and/or maximum balloon pressure cut-off of 150 kPa before urethral rupture (red dashed lines). Open circles indicate ruptured urethral samples. Filled circles indicate unruptured samples.
Internal urethral diametric strain and threshold maximum inflation pressures are important parameters for designing a safer urethral catheter system with lower intrinsic threshold inflation pressures. We have validated our porcine and cadaver findings in human male-to-female transgender urethral models and have recently implemented our safety device into clinical practice in Tallaght Hospital, Dublin, Ireland for patients requiring urethral catheterisation. This transition of a safety device from bench to bedside was commended during my presentation during March 2017, held at the European Association of Urology (EAU) congress, hosted in London, UK.





