BACKGROUND
Elastic arteries contain a high number of collagen and elastin filaments in their medial layer, providing the ability to stretch in response to ventricular contractions.1 The largest artery in the human body, the aorta acts as an elastic buffering chamber storing almost half of the left ventricular (LV) stroke volume during systole. In diastole, the elastic forces of the aortic wall release this residual volume to the peripheral circulation, thus creating a nearly continuous peripheral blood flow.2 With ageing, the elastic capacity of the aorta and the large arteries decreases, which leads to an increased cardiovascular risk.3 Therefore, the assessment of aortic elastic properties stands at the intersection of cardiovascular research, diagnosis, and risk stratification.4 CT has emerged as a valuable and reproducible method for the assessment of aortic elastic properties for risk stratification. The team aimed to compare the aortic elastic properties acquired by coronary CT angiography (CTCA) in patients with obstructive and non-obstructive coronary artery disease (CAD), and evaluate the association between aortic distensibility and obstructive CAD.
METHODS AND RESULTS
In this observational prospective study, consecutive patients undergoing CTCA for suspected CAD with low-to-moderate risk between September 2022–June 2023 were considered eligible. Image acquisition was performed through CCTA using an ECG-gated CT scanner (SOMATOM go.Top, Siemens Healthineers, Erlangen, Germany) according to the protocol recommended by the Society of Cardiovascular Computed Tomography (SCCT). Vessel analysis software (syngo.via, Siemens Healthineers) was used to quantify the area of ascending and descending aorta through the cardiac cycle. Aortic distensibility in the segment of ascending and descending aorta was calculated using the following formula: AD=ΔA/(Ad*ΔP), (AD, ×10-3 mmHg-1), where ΔA is the difference between the maximal luminal measured area and the minimal luminal measured area, and ΔP is the difference between systolic pressure and diastolic pressure. Patients were divided into two groups based on the severity of the CAD: obstructive CAD when a stenosis ≥50% was noted, and non-obstructive CAD when a stenosis <50% or none was found. Of all 201 patients enrolled in the study, 115 subjects (57%) had ≥50% coronary stenosis, and the remaining 84 (43%) patients had non-obstructive or no coronary disease. Patients with obstructive CAD were found to be significantly older (60.8±11.1 years versus 53±12 years; p=0.009); more often males (60.5% versus 53%; p=0.021); had a higher prevalence of diabetes (21.1% versus 15.2%; p=0.014); atrial fibrillation (12% versus 6%; p=0.018); and lower ascending aortic distensibility (1.45±0.94 10-3 mmHg-1 versus 2.03±0.88 10-3 mmHg-1; p=0.019). Univariate regression analysis including patient demographic and clinical characteristics, as well as aortic elastic properties obtained, was performed to search for independent predictors of significant CAD. Factors that showed significant predictive value were included in multivariate regression analysis. The results showed that ascending aortic distensibility assessed by CT had significant predictive value for the presence of coronary disease (hazard ratio [HR]: 1.92; 95% CI: 1.14–3.23; p=0.001), along with patient age (HR: 1.03; 95% CI: 1.00–1.05; p=0.029) and the presence of diabetes (HR: 1.11; 95% CI: 1.04–1.26; p=0.009) (Figure 1).
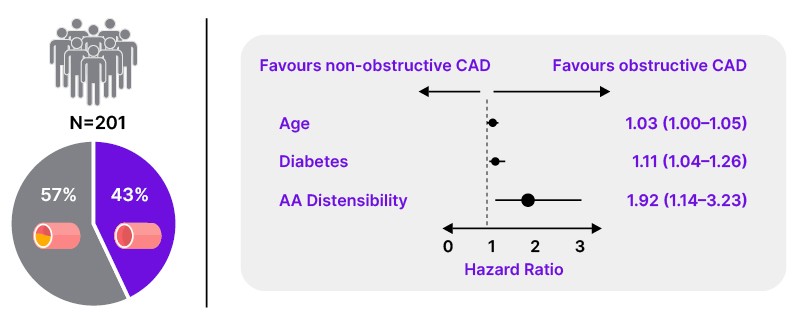
Figure 1: Predictive value of aortic distensibility for obstructive coronary artery disease.
AA: ascending aorta; CAD: coronary artery disease.
CONCLUSIONS
Evaluation of aortic elastic properties in patients referred for CTCA is feasible. Patients with obstructive CAD had lower distensibility of the ascending aorta. Furthermore, ascending aortic distensibility assessed by CT had significant predictive value for the presence of obstructive CAD.




