Abstract
Erection is a neurovascular response to visual, emotional, and tactile stimuli. It is classified as psychogenic, reflexogenic, and nocturnal. The causes of painful erections are Peyronie’s disease, penile fracture, penile tumours, penile lichen sclerosis, and a rare disorder called sleep-related painful erection syndrome. Here, the authors report six cases of painful spontaneous erection due to penile skin bridges in young males, seen between 2021–2023. They analysed the age, clinical features, treatment offered, and outcome at 3 months post-surgery. Patients’ mean age was 20.5 years (range: 13–35 years), and the haemoglobin genotype was AA. Two males had associated yellowish discharges under the skin bridges. They all had excision of the skin bridges with satisfactory post-operative appearance, and no pain with erection. Penile skin bridge is an uncommon cause of painful penile erection, and the authors recommend that all general practitioners be aware of this entity, and keep it in mind during a thorough physical examination.
Key Points
1. Penile skin bridge is a complication of neonatal circumcision. Therefore, meticulous circumcision must be practised.2. Penile skin bridges should be considered an uncommon cause of painful spontaneous penile erection in young males.
3. Surgical excision of skin bridges can provide a satisfactory cosmetic and functional outcome.
INTRODUCTION
Erection is a neurovascular response accompanied by the release of neurotransmitters. The penis is innervated by autonomic (sympathetic and parasympathetic) and somatic (sensory and motor) nerves. The neurons in the spinal cord and peripheral ganglia give rise to the sympathetic and parasympathetic nerves, which form the cavernous nerves that innervate the corpora cavernosa and corpus spongiosum, to stimulate the neurovascular activity during erection and detumescence.1,2
Stimulation of the pelvic parasympathetic nerves and cavernous nerves causes the release of nitric oxide (NO) and acetylcholine. NO mediates the activation of cyclic guanosine monophosphate that results in the downstream activation of protein kinases leading to sinusoidal relaxation, arterial dilatation, and venous compression. The stimulation of the sympathetic nerves inhibits norepinephrine release. Furthermore, stimulation of the somatic nerves releases acetylcholine, which reenforces the penile contraction. The somatic nerve is responsible for sensation, and the contraction of the bulbocavernous (needed for ejaculation) and ischiocavernous muscles (produces rigid erection). Both the autonomic and somatic nerves are activated at the spinal cord level (T11–L2, and S2–S4), and at tactile stimulation of the external genitalia. Nocturnal erection takes place during rapid-eye-movement (REM) sleep. Therefore, erection requires an intact brain with three components: visual stimuli (inferior temporal cortex), emotional/motivational component (paralimbic areas), and physiological component (controls endocrine and autonomic function in the left anterior cingulate cortex). There are three types of erection: psychogenic, reflexogenic, and nocturnal.1
Anatomically, the penis comprises three erectile tissues: right and left corpora cavernosa, and corpus spongiosum. The corpora cavernosa are surrounded by a rigid, tough bilaminar tunica albuginea. The three erectile tissues are covered by a thin fibrous tissue called the Bucks fascia, and all these structures are surrounded by the dartos fascia (subcutaneous areolar tissue) and penile skin. The corpus spongiosum expands distally to form the glans penis. The vascular supply to the erectile tissues is the cavernous artery and veins, which are branches of the internal pudendal vessels. The penile skin is supplied by the dorsal artery of the penis that is derived from the external pudendal artery. The cavernous vein communicates with the emissary veins through the subtunica venous plexus, and these veins are compressed during erection.3
Abnormality with adequate arterial and venous return during erection may result in persistent painful erection, especially in ischaemic priapism;2,4 as well as penile fracture that occurs during sexual intercourse, when the penis slips outside the vagina, and hits the inferior pubic rami bone.5,6 There is an association between lichen sclerosus et atrophicus and penile cancer. Lichen sclerosus is a benign, chronic, sclerosing atrophy of the glans and foreskin. It was reported in a 36-year-old male with whiteish atrophic patch on the glans penis, telangiectasia, and superficial ulcer associated with painful erection, which turned out to be an aggressive squamous cell tumour of the penis.7 Painful nocturnal erections, or sleep-related painful erections that occur during REM sleep, have been reported. This is found in young males, and has a common mean age of onset of 40 years.8
Skin bridges, a complication of circumcision, which commonly accompanies childhood circumcision, have been reported to cause tethering of the penis and occasional pain.9 The literature search in Nigeria, North Africa, East Africa, and South Africa did not reveal any previous publication on the relationship between penile skin bridge and erection in young males.
The authors present cases of post-circumcision penile skin bridge as an uncommon cause of painful erection in young males.
METHOD
Following the first case of a 17-year-old male who presented with painful spontaneous erection and yellowish discharge around the junction between distal penis and glans penis in 2021, the authors subsequently collected data from patients who presented with painful spontaneous erection, in the absence of sexual stimulation, and were managed over a 3-year period (2021–2023). The data included the age, clinical features, treatment offered, and outcome of treatment.
RESULTS
Six young males were managed for painful spontaneous penile erection. They were ages 13, 16, 17, 19, 23, and 35 years. The mean age was 20.5 years, with a range of 13–35 years. They all presented with erection, without sexual arousal, that was associated with pain, and two had yellowish discharge around the corona of the penis. There was no significant medical or surgical history apart from the neonatal circumcision that they all had; neither was there any genital trauma. They were not sexually active, except the 35-year-old who was afraid of engaging in sexual intercourse because of the painful erection.
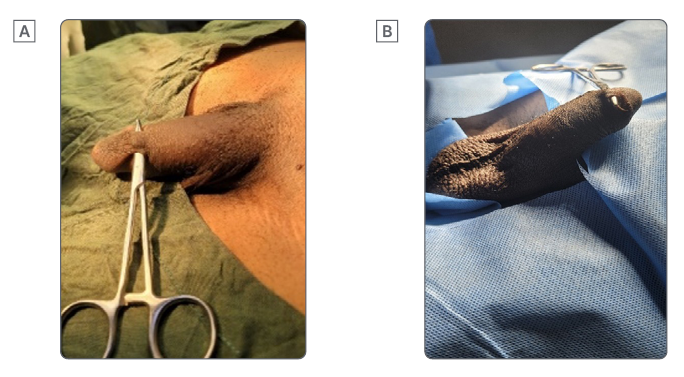
Figure 1: Pre-operative A) dorsal and B) ventral penile skin bridges.
The examination confirmed a circumcised male penis with multiple skin bridges around the dorsal, lateral, and ventral aspect of the penile corona (Figure 1A and 1B). Discharges (smegma) around the penis were seen in two patients (Figure 2A). Their haemoglobin genotype was AA. Pre-operative full blood count and urinalysis were essentially within the normal range. All patients had excision of the skin bridges under general intravenous anaesthesia, spinal anaesthesia, and local anaesthesia with sedation (Figure 2B). At 3 months post-surgery, the cosmetic appearance of the penis was satisfactory (Figure 3), and there was no pain with subsequent spontaneous penile erection.
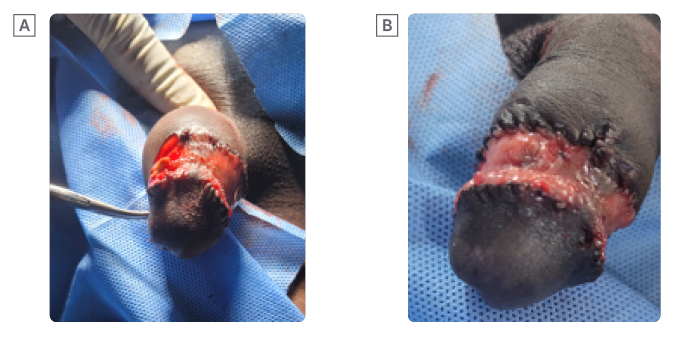
Figure 2: Intra-operative A) smegma and B) excised penile skin bridges.
DISCUSSION
Painful penile erection in adults implies persistence of venous obstruction and disruption of tunica albuginea, manifesting as acute priapism and penile fracture. Priapism is the sudden, persistent, often painful, purposeless penile erection that is not related to sexual arousal or ejaculation. The commonest cause of ischaemic priapism in 50% of cases is sickle cell disease. Other causes are the use of aphrodisiacs (19.2%), leukaemia (7.7%), and idiopathic (23.1%).4 Recurrent ischaemic priapism is another terminology for stuttering priapism, which is defined as repeated ischaemic episodes over time, and is self-limiting.2

Figure 3: Post-operative cosmetic functional penis.
Penile fracture is a sudden disruption of the tunica albuginea of the penis that often follows sexual intercourse in 48% of cases, where the penis slips out of the vagina and hits the pubic bone, or during masturbation and forced flexion of an erect penis in 39% of cases.5,6
Burnett8 described two rare causes of painful penile erection: painful nocturnal erection and sleep-related painful erection (SRPE), and idiopathic stuttering priapism. SRPE occurs during REM sleep, and is classified as parasomnia, which is a group of undesirable physical phenomena, such as movements/behaviours, or experiences of emotions, perceptions, and dreams that are seen while falling asleep, being asleep, or while waking up from sleep. SRPE affects males of all ages, with an average age of onset of 40 years.8
A separate subcategory of ischaemic priapism that is recurrent and idiopathic is termed idiopathic stuttering priapism. It is of short duration, recurrent, and believed to be stimulated by psychic centres, and manipulation of external genitalia.8
In this study, the authors report spontaneous penile erection in young males, due to skin bridges on the corona of the penis. These act as band-like vascularised tissue, and are a complication of neonatal circumcision, seen in all patients who were circumcised. These areas of adhesion between the glans and skin of the penile shaft prevent adequate elongation of the penis, and ultimately result in an abnormal curvature of the penis that is painful in these patients, as also previously reported by Kampouroglou et al.9 Kamal et al.10 documented the management of 57 adult males in Saudi Arabia who presented with penile skin bridges following childhood circumcision.
Two patients in this series presented with a yellowish discharge under the penile skin bridge. This was smegma, which is commonly found in uncircumcised males, but Almutawa et al.11 reported this in a 36-year-old, circumcised male. Smegma is an opaque white or yellowish substance composed of dead cells and skin oils that is malodorous.11
The penile skin bridge, when thick, is often vascularised. The treatment in this series was surgical excision.8,10,11 All patients were satisfied with the cosmetic appearance and function of their penis, with disappearance of pain with subsequent erection. Meticulous suturing and dressing at the time of circumcision can reduce the occurrence of penile skin bridge.
CONCLUSION
Penile skin bridges are an uncommon cause of painful erection, among others, and the authors recommend that all general practitioners be aware of this entity, and to keep it in mind during a thorough physical examination.





