
BACKGROUND
Nodular lymphocytic predominance Hodgkin lymphoma (NLPHL) is a very uncommon subtype of Hodgkin lymphoma (HL), representing approximately 5% of all HL cases, with an incidence of 0.3/100,000 cases per year and with unique characteristics that distinguish it from classic HL.1 The tumour cell that defines it, which the presence of is a requirement for diagnosis, is a malignant cell that was reclassified by the World Health Organization (WHO) 2008 as predominantly lymphocytic cell, and is also known by the more descriptive term of ‘popcorn’ cells.2
Given its low frequency, it becomes difficult to perform randomised studies, with the accumulated experience of academic groups being the main source of relevant information for the management of these patients.3
METHODS
In the study, 85 patients recruited by the Spanish Lymphoma Study Group (GOTEL) from 12 different hospitals and diagnosed between January 1970 and December 2015 were retrospectively analysed in order to describe their clinical and sociodemographic characteristics, survival rates, and causes of death.
RESULTS
The mean age of the study group was 37 years (range: 18–88), with 76.5% being male. Baseline characteristics are summarised in Table 1. Patients received different modalities of first-line treatment; the mean time to relapse was 3 years and 47% presented relapses beyond 5 years (higher probability in Stage IV; p<0.001). A total of 31% of tumour relapses were found, 77% of which were in 3/4 (75%) patients who did not receive any type of treatment, 7/15 (47%) that received only chemotherapy treatment, 12/43 (27%) who received radiotherapy, and 6/23 (26%) who received both chemotherapy and radiotherapy (26%).
The median follow-up was 16 years, with a 10-year overall survive of 92.9% and 81.2% at 20 years (Table 1). The overall lymphoma-specific survival was 98.8% at 10 years and 96.5% at 20 years, without significant differences between sex. It was evaluated whether survival differed depending on the time of treatment, before or after 1990; nonsignificant differences were found.
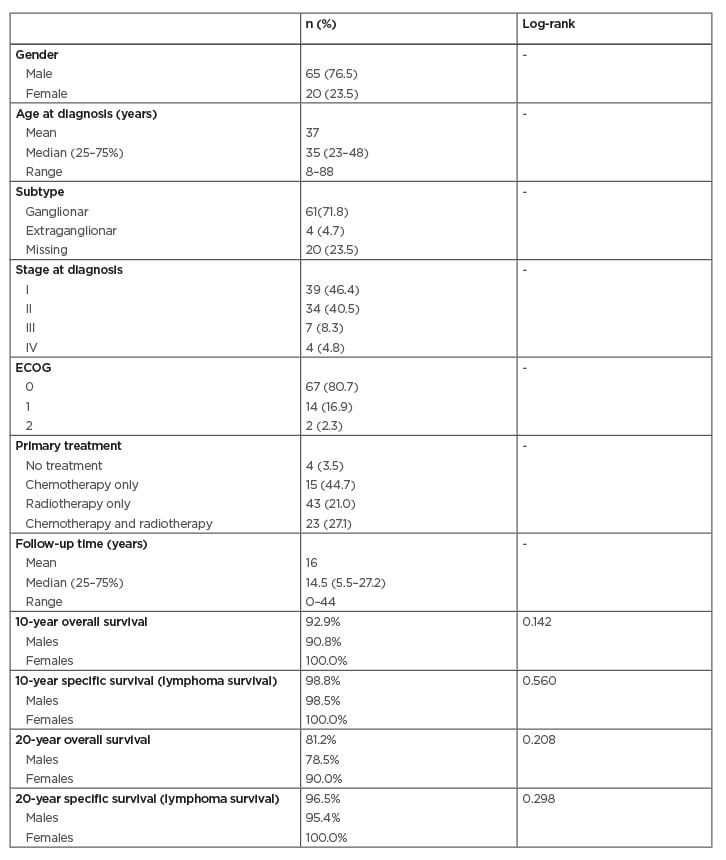
Table 1: Baseline characteristics and survival rates.
Of the 22 patients who had died by the time of analysis, only three died because of the primary lymphoma. There were five patients who developed a second tumour: two breast cancer (at 19 and 26 years from initial diagnosis), two head and neck cancer (at 7 and 5 years), one leukaemia (10 years from diagnosis). There were no patients who developed transformation to another more aggressive lymphoma.
CONCLUSIONS
The low prevalence of NLPHL makes the development of prospective randomised studies very difficult. The authors’ series is one of the longest follow-ups of NLPHL published, including extensive clinical information and specific causes of death. This work confirms the excellent prognosis of NLPHL, with high cause-specific survival rates and a very infrequent rate of NLPHL transformation. Given the high cure rates, treatment should be selected considering toxicity and side effects and could be adapted with early-stage radiation therapy when possible.






