
BACKGROUND AND AIMS
Chronic kidney disease (CKD) is a significant risk factor for preeclampsia (PE).1 However, the features of PE in this cohort of patients (pts) have not been previously studied in detail.2,3 In this regard, the analysis of PE in pts with CKD is of great clinical and social importance. The aim of the study is to analyse the incidence and characteristics of PE in pts with CKD.
MATERIALS AND METHODS
A retrospective analysis of 60 case histories of pregnant pts with CKD (Stages 1–4) was carried out, 27 of whom had CKD Stage 3a–4. Ten (37%) patients with CKD 3a–4 developed PE, then the course of their pregnancy was analysed. Creatinine level (Scr), proteinuria (PU), and blood pressure (BP) were assessed at the time of the first visit to the centre and at the time of PE. The physiological response of the kidneys to pregnancy as a decrease in Scr by 10% of the pregestational value was assessed in six pts with Scr values known before pregnancy.
RESULTS
In the group of pts with PE and advanced CKD, the mean age was 32.3 (±4.8) years (range: 28– 42 years). The most common cause of CKD was glomerulonephritis (6; 60%), and one each for tubulointerstitial nephritis, diabetic nephropathy, aHUS, and APS-associated nephropathy. Four pts had CKD C3a (40%), three had C3b (30%), and three had C4 (30%). The mean term of gestation at the time of first visit to nephrologist was 15.6 weeks. At the first measurement during pregnancy, the mean Scr was 157 (±69) μmol/L; the physiological response of the kidneys to pregnancy was noted only in one out of six pts. The mean PU was 1.2 (±0.8) g/L. Three pts had arterial hypertension (30%) and only one patient received antihypertensive therapy before pregnancy with the achievement of target BP values. The mean BP values at the first visit were: SBP 131 (±11.5)/DBP 84 (±7.3) mmHg. Aspirin for the prevention of PE was prescribed in a timely manner in six cases (60%); in other cases, aspirin was either not prescribed or was added to therapy after 12 weeks of pregnancy. Of 10 pts with PE, 7 (70%) pts developed early PE (before 34 weeks of gestation); the median term for the development of PE was 31.3 weeks (27–36.5). The mean BP values at the moment of PE were 142 (±17)/90 (±10.6) mmHg. The majority of pts showed an increase in PU (Table 1). Increase in Scr was observed in six (60%) pts (Table 1). Another sign of a severe course of PE was thrombocytopenia in two cases (<100,000 in 1 μL), in one case as the symptom of HELLP syndrome. The markers of PE (sFlt1, PLGF, sFlt1/ PLGF) were analysed in 5 (50%) cases. The mean value of the ratio at the moment of PE was sFlt1/ PLGF:157.6, which, for a given gestational term (31.3 weeks), corresponds to severe ischaemic damage to the placenta.
The mean delivery term was 32.4 weeks of gestation; all newborns were alive and viable with the mean weight 1,514 g (978-2,250 g).
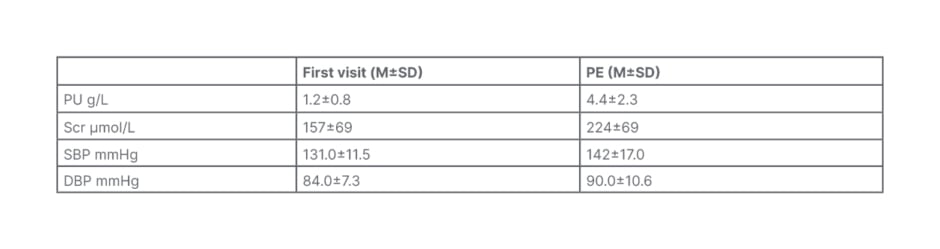
Table 1: Сlinical data of female patients with chronic kidney disease and preeclampsia.
DBP: diastolic blood pressure; M: mean; PU: proteinuria; SBP: systolic blood pressure; Scr: serum creatinine; SD: standard deviation.
CONCLUSION
According to study data, the incidence of PE in CKD Stages 3a-4 was 37%. The main features of PE in pts with advanced CKD were its early onset, severe course with kidney damage in 60% of cases, and relatively low BP values. ●






