
Abstract
Penile size is a frequently observed concern in men of all ages. The way in which some men see their personality is defined, appraised, or reflected by their penis, with the view that ‘bigger is better’, is termed ‘phallocentrism’. In this review article, we assess the literature and evaluate the evidence on what is ‘normal’ in relation to penile size, and evaluate techniques for penile lengthening and girth augmentation with emphasis on the possible benefits and complications of the procedures reviewed.
INTRODUCTION
The penis has been regarded as a symbol of masculinity throughout history, hence penile size has long been a source of anxiety for many men. Though the majority of men fall within the ‘normal’ range of penile length, the concerns regarding penile size and girth may cause low self-esteem, sexual dysfunction, depression, and other psychiatric disorders.
For centuries, men have undergone many different processes in an effort to enlarge and enhance their penises. For instance, the Sadhus, holy men of India, and men of the Caramoja tribe in Uganda use weights to increase the length of their penises. The men of the Dayak tribe from Borneo were the first to introduce penile piercing, inserting decorations for their partner’s pleasure.1 Evidence suggests that the ancient Greeks and Romans also fixated on the penis and its importance; this can be observed in some of the paintings and statues from that era.2
The tendency of some men to look for their identity in their penis with the view that ‘bigger is better’ is reflected by the term ‘phallic identity’, as introduced by Vardi, or ‘phallocentrism’.1,3 The notion of small penises and the influence of different media on sexual issues, which just a few decades ago were considered taboo and socially unacceptable for discussion in public, has led to the development of a number of different modes of penile enhancement. Because of this, the psychiatric term ‘penile dysmorphophobia’ was introduced to describe an abnormal perception of penile size, when the penis itself is within what is considered to be the normal size range.4
METHODS
We searched the MEDLINE database for articles describing various techniques for penis enhancement using the following keywords: penis, small penis syndrome, penile enhancement, penis augmentation, penis lengthening, and penile reconstruction surgery. Only articles written in the English language were included; articles in which the only recommendation for penis augmentation was phalloplasty using extragenital tissue were excluded.
REVIEW
Penile Size
The question of what is considered a ‘normal’ penile size has remained ambiguous, lacking a consensus until recently. Recently, there have been several studies published on penile length and girth and what should be considered a normal penis size or a micropenis.
The first studies to address penile size were published in the 19th century, and the publication of such articles continued thereafter.2 The authors of these studies measured various aspects of penis size, including penis length in flaccid, flaccid stretched, and erect states, and penile girth in both flaccid and erect states. The variability of the recorded values depended on the population included in the study, as well as on the measuring technique.5 In these studies, average penis length was estimated to be approximately 9 cm when flaccid, and ranged from 12–13 cm and 14–16 cm in flaccid stretched and erect states, respectively. In regard to girth, the average circumference ranged from 9–10 cm when flaccid and from 12–13 cm in the erect state.2,5-10
The studies presented demonstrated that younger men usually have longer, wider penises.9 One study also showed a large statistical difference between homosexual and heterosexual men in terms of penis girth and length, with homosexual men reporting larger penises than heterosexual men.11 There remains a need for further investigation of penis size among different races, as there are a lack of studies focussing on this aspect.
Unbiased standardisation is needed to make the comparison of data more accurate. In all cited studies, we saw differences in the technique used to measure penis size. There now exists a general consensus that penile length should be measured on the dorsal side of the penis, from the penopubic junction to the tip of the glans in the flaccid, flaccid stretched, and erect states. Likewise, penile girth should be measured around the middle of the shaft of the penis in both the flaccid and erect state. The measurements should be made by a single physician and should not use self-reported questionnaire data. With the exception of Wessells’ records,9 no study performed these measurements under all of these conditions. Given the huge variability in penile size and penile extensibility, penile evaluation should, without a doubt, be performed in flaccid and stretched states, with the specific final objective of reaching a consensus on the definition of what penile size encompasses and the associated method of measurement. After considering these studies, Dillon et al.2 concluded that with respect to penile length, average flaccid penis size was approximately 9.0–9.5 cm, and 14.5–15 cm in the maximally stretched state. Average erect penis length ranged from 12.8–14.5 cm, and girth approximately 10.0–10.5 cm. By applying these findings, we were able to define potential candidates for penile enhancement surgery as men who are two standard deviations below the average size, and patients with a flaccid penile length of <5 cm and girth <8 cm.2
Micropenises
The term micropenis refers to a series of congenital and acquired conditions that result in an abnormally short penis; this state can be associated with functional and psychological problems.12
A true micropenis results from hormonal disruption during gestational development and results in either an isolated micropenis, or a micropenis as part of a sexual development disorder.13 The hormonal causes of micropenis development can be classified into three groups: hypogonadotropic hypogonadism, hypergonadotropic hypogonadism, and idiopathic hypogonadism.13 As patients with a true micropenis can also suffer from emotional and psychological crises due to the functional problems associated with small penis size, a multidisciplinary approach is essential for diagnosis and treatment. All patients in whom there is a suspicion of a micropenis condition should undergo karyotyping and hormonal evaluation, as well as a detailed examination by an endocrinologist. Nonsurgical treatment of the true micropenis in infancy involves the correction of reversible metabolic defects. However, surgical treatment such as gender reassignment or penis augmentation surgery in childhood should be carefully evaluated.12
The development of an acquired micropenis involves penile shortening, which can occur as a consequence of diseases such as prostate cancer, priapism, Peyronie’s disease, erectile dysfunction, Fournier’s gangrene, lichen sclerosus, penile cancer, or trauma. Penile shortening happens as a result of corporal fibrosis due to chronic hypoxia, anatomical shortening, loss of tissue elasticity after penile surgery, creation of plaque in Peyronie’s disease, or after radical surgery for benign or malignant tumours. In many cases, reconstructive surgery offers patients a feasible option for restoring penis length and function (penile reconstructive surgery, grafting, penile prosthesis, etc.). Nevertheless, adequate counselling is necessary to create realistic post-operative expectations among these patients and to support their long-term rehabilitation.12
Ghanem et al.14 used a structured protocol for the management and counselling of 250 men who complained of a small penis size. Examination revealed that 81.6% patients had no physical abnormality and presented with a normal-sized penis. After application of a structured management and counselling protocol, 96.4% of patients agreed that their penis size concerns had been eliminated. Only nine patients decided to seek further surgical treatment. Of the nine patients who underwent penis augmentation surgery, only one true micropenis patient and two normal-sized penis patients were satisfied with the results of the surgery, with the remainder of the patients reporting poor satisfaction with the achieved size. The results of this study suggest that the majority of men complaining of a small penile size are misinformed, while some suffer from body dysmorphic disorder (BDD) in the form of penile dysmorphophobia. In this population of dysmorphic men, we can achieve better results through counselling and support from psychologists and psycho-sexologists, than by offering surgical augmentation.14
Penile Augmentation Procedures
There are several distinct types of penile augmentation surgery, each aimed at a different outcome; some increase length or girth, and a third group aims to achieve both of these objectives. In addition, there are several related plastic surgery procedures aimed at reconstructing the skin surrounding the penis. In a position statement draft regarding penis augmentation surgery, the Sexual Medicine Society of North America has concluded that penile lengthening and girth enhancement surgery can only be regarded as experimental surgery, as there are no peer-reviewed, objective, or independently monitored studies or other data that prove the safety or efficacy of penis lengthening and girth enhancement surgery.2,15
As Ghanem et al.14,16 state, many men complaining of small penis syndrome (SPS) have a misconception of what normal penis size is, but there are also those who suffer from BDD. In all of these patients, education regarding normal variations in penile size is very important, as is psychotherapy.14,16 In cases in which the patient is still considering surgery after completing psychological counselling, there are several surgical options available which will be reviewed in this article.
Penile Lengthening
Several techniques have been described to increase penis length. Some patients complain of SPS as a result of abundant suprapubic fat tissue or a protruding abdomen, which can be solved by liposuction and/or suprapubic lipectomy. This achieves a visual lengthening of the penis.1,17,18 In cases where the patient requires further penile lengthening, one proposed surgical technique is to detach the suspensory ligament of the penis. Dissection of the suspensory ligament enables the penis to move forward and to appear longer in the flaccid state by 1.5–2 cm. Reattachment of the ligaments and de novo penile shortening need to be avoided. Alter et al.19 recommend suturing the vascularised flap from the lipomatous tissue of the spermatic cord to the pubic periosteum, and Li et al.20 suggest suturing a small silicone testicular prosthesis to the base of the pubis to prevent penile retraction.1,19,20 All authors recommend the use of special penile extenders to keep the penis separated from the pubis, which also allows the penis to heal in the most extended position possible.
This procedure is often combined with inverted V-Y plasty or Z-plasty to increase penile length further, or use of the circumcision approach to prevent visible scarring on the lower abdomen.21 Inverted V-Y plasty was first described by Long, and later modified by Roos and Lissoos22 in 1994. They described the use of suspensory ligament release resulting in an increase in length of 4 cm in their group of patients.1,22 Lower abdominal Z-plasty produces the best results due to low risk of scrotal skin sliding onto the penile shaft.19 The role of a suspensory ligament is very important in penile stabilisation during erection to create a specific angle for vaginal penetration and sexual intercourse; dissection of the ligament can lead to a downward position of the penis in the erect state.
In patients with penoscrotal webbing that results in a hidden penis, the reconstruction of the penoscrotal angle and scrotal and penile skin by Z-plasty can resolve the problem without additional procedures for penile lengthening. In 2007, Alter23 reported that overly aggressive circumcision in which too much ventral penile skin is excised results in penile shortening due to penoscrotal webbing in the majority of patients.
In 2000, Perovic and Djordjevic24 reported penile lengthening in 19 patients using the penile disassembly technique, a technique involving the placement of the autologous rib cartilage between the corpora cavernosa and glans cap; however, long-term follow-up data are not available.24
A special group of patients requiring penile elongation procedures are those with epispadias and bladder extrophy.2 These patients receive surgery to repair the bladder and penis during early childhood and are monitored by paediatric urologists. The most commonly used procedure for epispadias repair is the Cantwell–Ransley staged procedure.25 In rare cases, patients report short penises with severe dorsal penile curvatures and short urethras that require secondary repair. In 2013, Djordjevic et al.26 reported good functional and cosmetic results in 19 of 23 patients with failed epispadias repair in childhood, with an improvement in penile length of 2.7–6.6 cm in the erect state.26
Penile Girth Enhancement
Penis girth enhancement procedures are even more controversial than penis lengthening procedures. There is no standardised recommendation or indication for penile girth enhancement in the medical literature, and no guidelines have been proposed for such an intervention.2,8 The goal of such a procedure would be a symmetrical increase in the girth of the penis, and though there is no standardised process, methods with this objective have been described and used either by patients themselves or by doctors such as plastic surgeons, urologists, and dermatologists.
Instillation of different exogenous substances under the skin for penile girth enlargement is very common in some culture settings and is present even today.27 Injection of liquid and melted paraffin was introduced around the year 1900 to enlarge penis circumference. Paraffin injection causes an intense inflammatory reaction leading to granulomas, ulcers, and skin necrosis, with the risk of penis loss (Figure 1).28,29
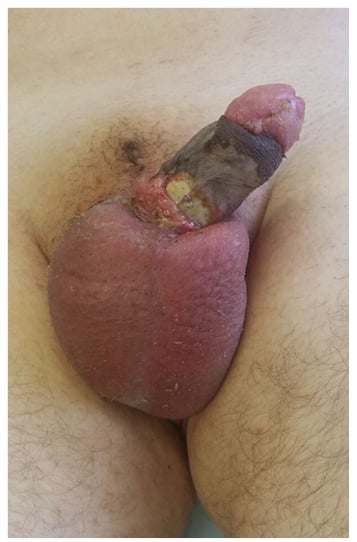
Figure 1: Severe penile skin necrosis after penile enhancement with paraffin injections.
Liquid injectable silicone (LIS) became very popular in aesthetic surgery in the 1940s and appeared to be relatively safe.30 Inspired by early results, surgeons started injecting LIS for penile girth enhancement but stopped following the appearance of silicone migration and the development of complications such as erectile dysfunction, significant and prolonged swelling, penile curvature, and late granulomatous reactions.31,32 However, despite the side effects, Yacobi et al.33 reported full short-term satisfaction in 324 patients injected with LIS with an average augmented penis circumference of 2.6 cm.
Injection of autologous fat was initially thought to be a promising procedure for penis girth enhancement. Panfilov34 reported a mean girth enhancement of 2.65 cm in 88 patients following the injection of 40–68 mL of autologous fat. Following this, in 2012, Kang et al.35 reported an average increase in girth of 2.71 cm following injection of 25–49 mL of autologous fat. There are fewer complications associated with the injection of a small amount of fat tissue with a minimal increase in girth compared with the injection of larger amounts. Increasing the amount of injected fat results in a more significant immediate girth enhancement, but is also associated with a much higher risk of complications. It has been proven that >50% of injected fat is absorbed, and the injection of large amounts can cause severe penile deformities, necrosis, and calcification of the fat tissue, as well as asymmetry.1,19
Kim et al.36 reported satisfying results in an 18- month follow-up of 15 men treated with polymethyl methacrylate and cross-linked dextran for penile augmentation without side effects or migration of the instilled material. Further follow-up and larger series of patients are needed to prove the safety of this penile enhancement procedure.36
After observing the developments in aesthetic surgery, urologists and plastic surgeons started to use injectable hyaluronic acid gel for penile and glans augmentation.37 Perovic et al.38 reported good results of enlargement and sculpturing of small and deformed glans in 8 of 9 patients who were subjected to this technique. The authors did not report any side effects from the hyaluronic acid gel. In same year, Kim et al.39 reported a high satisfaction rate among 187 men who underwent this glans enlargement procedure with an increase in glanular circumference of 1.5 cm at 1-year follow-up. Kwak et al.40 followed 38 patients for a period of 5 years and did not report a significant difference in patients’ visual estimation of glans circumference. The advantages of hyaluronic acid gel are increased tissue longevity and possible reinjection in cases of long-term volume loss, with few studies’ reporting immediate or delayed adverse effects in association with its use.
Another advancement is the use of dermal fat grafts, which, according to Alter,19 are considered to be superior to the fat injection procedure and have been used with success in plastic surgery. Alter also states that circumferential placement of the dermal graft without covering the urethra is the ideal technique with an average girth enhancement between 2.5–5 cm.19 Nonetheless, inadequate graft harvesting, local infection, graft fibrosis resulting in penile curvature, and subsequent shortening made this technique unacceptable for penile girth enhancement. These findings opened the door to other researchers in this field to present their techniques.17
In 2002, Austoni et al.41 performed bilateral saphenous graft augmentation of the penis in 39 patients with penile hypoplasia or penile dysmorphophobia. Shaeer et al.42 have recently reported superficial circumflex iliac artery and vein flap as a reliable option for long-lasting and sizeable penile girth augmentation. However, these procedures are thought to be an invasive and aggressive treatment for patients with penile dysmorphophobia.
The use of acellular inert dermal matrices (allografts) is common in plastic surgery, especially in breast reconstruction. The use of allografts in penile girth enhancement surgery is believed to have potential in providing good cosmetic results with respect to penile symmetry and durability, and to present with a lower complication rate compared with the dermal fat graft technique. The technique includes placement of the allograft around the penile shaft at the level of the deep fascia of the penis. However, in a study by Solomon et al.43 20 patients developed a graft infection, which was either treated solely by antibiotics or required additional surgery, while 3 patients suffered graft loss. Due to the lack of new data on allograft use in penile girth enhancement, this procedure still needs to be considered experimental.1
Development of tissue engineering also led to its use in penis girth enhancement. We published the use of poly(lactic-co-glycolic acid) (PLGA) scaffolds pretreated with autologous fibroblasts for penis girth enhancement.44 The pretreated scaffolds were placed between the dartos and deep fascia without covering the urethra following penile degloving. Of the 84 patients who entered the study, 70% were completely satisfied. Mean penile girth augmentation was 3.15 cm in the flaccid state and 2.47 cm in the erect state (Figure 2a, 2b, and 2c).45 Complications included local infection, local skin necrosis, and seroma, which were treated conservatively. During the repeat procedure, we obtained samples of newly formed tissue 9–12 months after previous penis girth enhancement with PLGA-pretreated scaffolds. Microscopic evaluation showed the presence of vascularised loose connective tissue with an abundance of collagen fibres, fibroblasts, and inflammatory cells, indicating active neovascularisation and fibrillogenesis.46 Jin et al.47 obtained similar results after treating 69 patients with SPS, of which 94.2% were satisfied with the procedure. Further studies and long-term follow-up are also needed for this treatment.
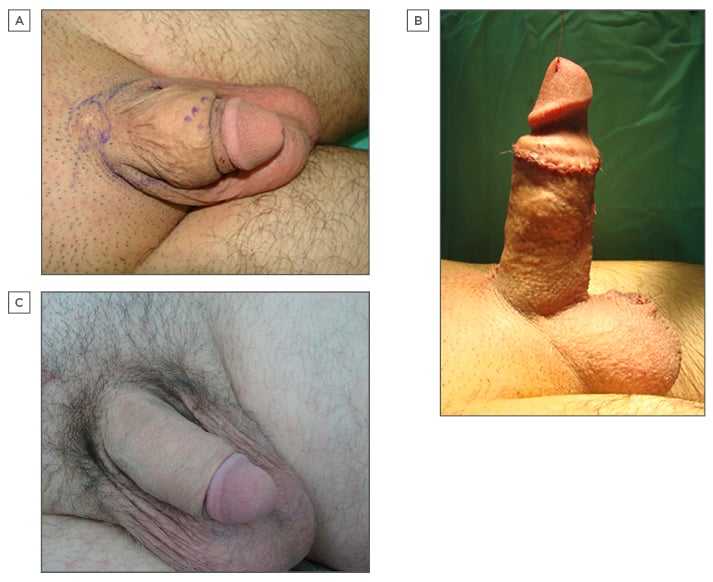
Figure 2: Penile enhancement by poly(lactic-co-glycolic acid) scaffolds.
A) Outcome after penile enlargement by lipofilling. Penis is shortened and deformed; B) Appearance after redo surgery: two poly(lactic-co-glycolic acid) scaffolds pretreated with autologous fibroblasts are placed around the penile body. Penoscrotal webbing is corrected; C) Appearance at 6-month follow-up: good contour of the augmented penis is achieved. Difference before and after surgery is clear.
CONCLUSION
The topic of penile size is a contentious issue for many men, regardless of their age. Penis size is considered a symbol of masculinity and sexual power and has great impact on self-esteem and sexual function. Based on the current status of science, penis enhancement surgery is still considered to be experimental and its indications are still a matter of medical and ethical debate.
As there is still a significant percentage of patients that are dissatisfied following penis enhancement procedures, preoperative counselling with a psychologist and sexologist should be considered to moderate patients’ expectations from penis augmentation surgeries. In this respect, we believe that tissue engineering presents a new opportunity in penis augmentation surgery that should be developed in the future.





