
BACKGROUND AND AIMS
Retrograde ureteroscopic endopyelotomy is an alternative treatment of short (<1 cm) ureteropelvic junction (UPJ) obstruction. In current literature, the use of holmium laser (AurigaTM, Boston Scientific, Massachusetts, USA) for this kind of surgery is still not widely described. With regard to the thulium fiber laser (FiberLase U1®, IRE-Polyus), there is limited similar data. Recently, the authors reported initial results of thulium fiber laser application for UPJ stricture management.1 The advantage of thulium laser application is low penetration depth (0.2 mm) while obtaining a controlled and safe tissue cut.2 Recent comparatives studies showed fewer favourable outcomes regarding endopyelotomy, compared with open or laparoscopic pyeloplasty;3 however, the role of thulium laser retrograde endopyelotomy should be investigated in more detail.
MATERIALS AND METHODS
In this study, the authors evaluated the efficacy and safety of endoscopic retrograde UPJ stricture treatment with a thulium laser. A total of 94 patients with UPJ strictures treated at Pletnev City Clinical Hospital between 2015 and 2019 was retrospectively divided into two groups. The first group included patients who had been treated with retrograde laser endopyelotomy; the second group of patients had undergone laparoscopic dismembered (Anderson–Hynes) pyeloplasty.
Preoperative parameters were assessed: the nature of the stricture (primary or secondary, after failed treatment), the kidney function decrease, the presence of crossing vessels, the obstruction length, and renal pelvis dilatation. All patients in the first endoscopic group had no crossing vessels and presented with obstruction length <1 cm. The indications in both groups for intervention were pain, recurrent pyelonephritis, and concomitant upper tract stones.
RESULTS
There was a shorter operation time (24±14 min versus 82±2 min) and postoperative stay (2±1 versus 4±2 days) for retrograde thulium laser endopyelotomy patients in comparison to the laparoscopic group. One-year follow-up evaluation was undertaken for 36 patients from the first group, and for 29 patients from the second group. Two recurrences (4.2%) occurred in the first group, and one (2.2%) after laparoscopic surgery. The renal pelvis dilation decreased in 34 (94.4%) and 28 (89.6%) patients, respectively. The study demonstrated slightly better outcomes for laparoscopic pyeloplasty compared to laser endopyelotomy in terms of kidney function increase (89.6% versus 72.2% of patients experiencing any increase).
CONCLUSION
The authors presented their initial experience of thulium laser application for the treatment of retrograde UPJ stricture (Figure 1). Suggested indications for this treatment are primary or secondary UPJ stricture with length <1 cm, no crossing vessels, and renal pelvis dilatation ≤4 cm. Current literature supports endoscopic management of UPJ strictures for cases of previously-failed open or laparoscopic reconstructive surgery.4,5 As the next step of this study, the authors intend to recruit more patients and perform a 24-month follow-up of earlier treated patients. The authors consider the thulium fiber laser retrograde endopyelotomy to be a feasible and safe procedure for a variety of UPJ strictures.
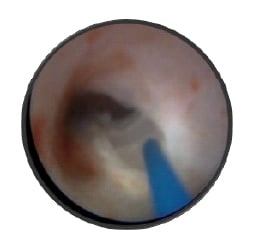
Figure 1: Retrograde thulium laser endopyelotomy in a patient with ureteropelvic junction stricture.
Surgery performed by Alexey G. Martov at Department of Urology, D.D. Pletnev City Clinical Hospital, Moscow, Russia, in 2019. Patient consent provided.





