BACKGROUND AND AIMS
Approximately 15–20% of patients who undergo urethroplasty (UP) with buccal mucosa graft (BMG) will suffer urethral stricture recurrence.1 The authors’ aim was to examine whether the stricture recurrence rate was influenced by reconstruction of the meatus (MR) during UP.
MATERIALS AND METHODS
The authors enrolled 1,954 patients with urethral strictures who underwent a UP using BMG from April 1994–April 2023 at their institution. Of these patients, 1,658 underwent a single-stage procedure (always ventral onlay). In cases of MR, a glans tunnelling was performed. Inclusion criteria were as follows: single-stage UP of the penile urethra (≤10 cm long; minimum distance to the sphincter: 5 cm), and no history of hypospadias. Advised follow-up was as follows: uroflow and residual urine (standing 3 months in the first 2 years, and then 6 months), and patient self-reported questionnaires on quality of life, morbidity, and satisfaction. In cases of maximum flow <20 mL/sec, residual urine >50 mL, or urinary tract infection, a urethroscopy and/or a urethrography were recommended. A stricture recurrence was defined as any instrumentation to the urethra during follow-up.
RESULTS
In 7.4% of patients (123/1,658), penile strictures were defined. The MR was performed in 46.3% of patients (57/123; Group 1). Group 2 (without MR) consisted of 44.7% of patients (55/123). The meatal involvement was unknown in 8.9% of patients (11/123). For patient characteristics see the table below (Table 1).
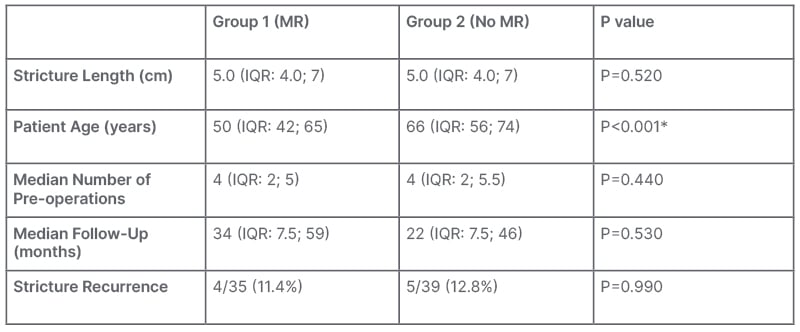
Table 1: Patient characteristics.
*Denotes statistical significance.
IQR: interquartile range; MR: meatus reconstruction.
From a total of 123 patients, data regarding stricture recurrence were available in 66.7% (87/123). Stricture recurrence occurred in 12.2% of these patients (10/82). There was no statistical difference between the two groups of patients.
Complications were observed in a total of 14.6% of patients (18/123), of whom 2.4% (3/123) were above Grade 3(*), according to Clavien-Dindo. In Group 1, three fistulas (one surgically treated*), three wound healing disorders, two cases of deep vein thrombosis, and one case of delirium, were observed across eight patients. In Group 2, one fistula, two wound healing disorders, three BMG-rejections on first miction voiding cystourethrogram, one penile deviation*, and one pulmonary embolism* were observed across eight patients. Two additional complications (one wound healing disorder and one BMG-rejection on first voiding cystourethrogram) occurred in patients in whom meatal involvement was unknown.
CONCLUSION
The reconstruction of meatus during urethroplasty with buccal mucosa graft does not influence the stricture recurrence rate. The patient undergoing this type of surgery should be informed that the most important complications are fistula formation, impaired wound healing, and deep vein thrombosis.





