
Treat-to-target principles in rheumatoid arthritis (RA) are now widely recognised as effective in achieving optimal disease outcomes. This study examined differences in outcomes between low (LDAS) and remission (RDAS) disease activity score (DAS) categories, addressing whether LDAS is an acceptable treatment target in RA.
Data from two consecutive UK multicentre RA inception cohorts with similar designs were used: the Early RA Study and the Early RA Network. Recruitment figures and median follow-up for the Early RA Study and Early RA Network were 1,465 and 10 years (maximum 25 years), and 1,236 and 6 years (maximum 10 years), respectively. Standard demographic and clinical variables were recorded at baseline and then annually until the end of study follow-up. Disease activity was categorised as remission (mRDAS <2.6) or low (mLDAS 2.6–3.2) using mean DAS 28-joint count (DAS28) score between Years 1 and 5; classification also included sustained low/remission DAS (sLDAS/sRDAS), based on DAS persisting in each of the two categories at Years 1–2, and Boolean remission (Years 1–2). Change in Health Assessment Questionnaire (HAQ) and 36-item Short Form Survey (SF36) (physical [PCS] and mental [MCS] components) for each disease activity category were modelled using linear mixed models with time incorporated as a linear spline with change-point at 12 months. Year of onset, age, sex, and use of steroids or conventional disease-modifying antirheumatic drugs at first visit were included as covariates. From a total of 2,701 patients across the two cohorts, 468 (17%) were in mRDAS and 284 (11%) in mLDAS in the first 5 years of disease. Lower proportions of patients achieved sRDAS (8%), sLDAS (6%), and Boolean remission (2%). Mean age was similar across categories but more women were in LDAS versus RDAS. Compared to mLDAS or sLDAS, inflammatory markers, DAS, functional (HAQ, PCS) scores, and mental (MCS) scores tended to be better in the mRDAS, sRDAS, and Boolean remission categories. Significant differences (p<0.05) were noted between the mRDAS and mLDAS between Years 1 and 5 for all outcomes; for sRDAS compared to sLDAS, the difference was significant at Year 1 but not by Year 5. Figure 1 shows disability (HAQ) and SF36 (PCS and MCS) for each disease activity category.
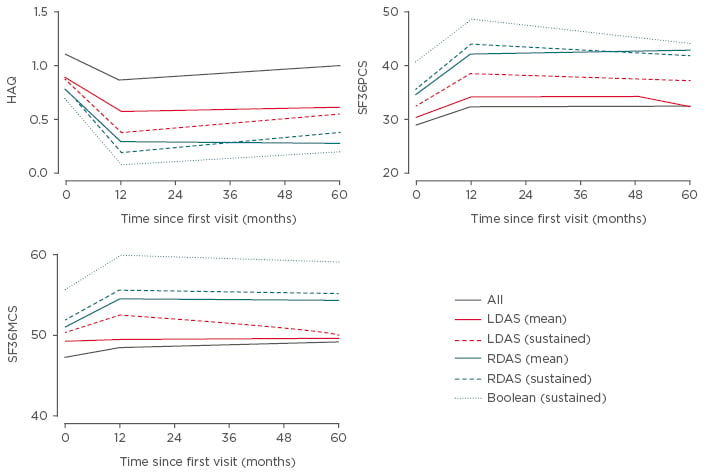
Figure 1: Health Assessment Questionnaire and 36-item Short Form Survey outcomes by disease activity category.
HAQ: Health Assessment Questionnaire; LDAS: low disease activity score; RDAS: remission disease activity score; SF36MCS: 36-item Short Form Survey mental component score; SF36PCS: 36-item Short Form Survey physical component score.
In summary, this study demonstrates striking differences between RDAS and LDAS categories, suggesting worse functional and SF36 outcomes over time in the LDAS categories. This is an important observation because it justifies striving for remission in RA to improve patient outcomes. The study therefore concludes that remission should be the primary treat-to-target goal in RA.






