Abstract
The authors present a case of a 77-year-old female, a former smoker with a history of chronic obstructive pulmonary disease who underwent bronchoscopy for evaluation of haemoptysis. The bronchoscopy revealed an anatomical variant of the right upper lobe bronchus with five branches instead of the usual three. This case report describes a peculiar anatomical abnormality in the right upper lobe. A review of the literature related to various variants in bronchial anatomy is presented.
Conclusion: Awareness of this anatomical variation provides valuable information to clinicians, particularly thoracic surgeons, to plan surgical interventions, tailor procedures, and minimise complications.
Key Points
1. Right upper lobe bronchus anatomical variations may be more common than previously thought, as they may be asymptomatic and therefore go undetected.2. Anatomical variations of the right upper lobe bronchus can lead to technical difficulties during diagnostic procedures, impact the distribution of inhaled medications, increase the risk of atelectasis or aspiration, and increase the risk of complications during surgery.
3. Radiologists and clinicians should be aware of tracheobronchial anomalies to ensure appropriate management of pulmonary disorders.
INTRODUCTION
There are various anatomical classifications of bronchial tree available in the literature, including the Jackson–Huber classification,1 the Yamashita Japanese classification,2 and the Boyden surgical anatomy classification.3 Contrary to these classifications, anatomical variance may exist that might show in a variety of ways, from being asymptomatic to exhibiting a variety of symptoms. Segmentectomies of the right upper lobe,4 as well as imaging, diagnostic and interventional endoscopy, brachytherapy, and anaesthetic tracheal intubation all require knowledge of these variances. Accurate diagnosis and effective care can be aided by close attention to not only radiological and bronchoscopy findings, but also anatomical variances. Here, the authors present a case with bronchoscopy revealing an anatomical variant of the right upper lobe bronchus with five branches, and its clinical implication with a review of the literature.
CASE REPORT
A 77-year-old female presented to the outpatient department of All India Institute of Medical Sciences (AIIMS), Patna, India, with a chief complaint of shortness of breath and cough for 45 days. She was a former bidi smoker, with a history of hypertension and exposure to biomass fuel. The patient also reported history of haemoptysis in past, one episode 25 years ago. She had taken anti-tubercular treatment for 2 years on an emperical basis around 25 years ago. Family history of bronchial asthma was present. Amlodipine was being used by the patient to treat hypertension. Theophyllines, oral bronchodilators, and antihistamines were also occasionally taken by the patient for symptomatic relief, with no prior history of using inhaled drugs, or any regular therapy for obstructive airway disease.
There were no relevant past interventions done as per patient’s recall, nor were there any records available. On further investigation, chest CT showed multiple sub-segmental areas of atelectasis surrounding ground-glass opacities, and sub-pleural fibrotic bands were observed, along with pleural thickening, and segmental and sub-segmental tractional bronchiectasis in bilateral upper lobes. Therefore, the authors proceeded to fiberoptic bronchoscopy to evaluate for any obvious site of bleeding, and to rule out infections. Although infective aetiology was ruled out, no obvious site of bleeding could be appreciated during the procedure. An uncommon anatomical variant of right upper lobe bronchus, with the right bronchus intermedius normal in its anatomy branching into the right middle and lower lobe bronchus segments (Figure 1), was observed during the procedure.
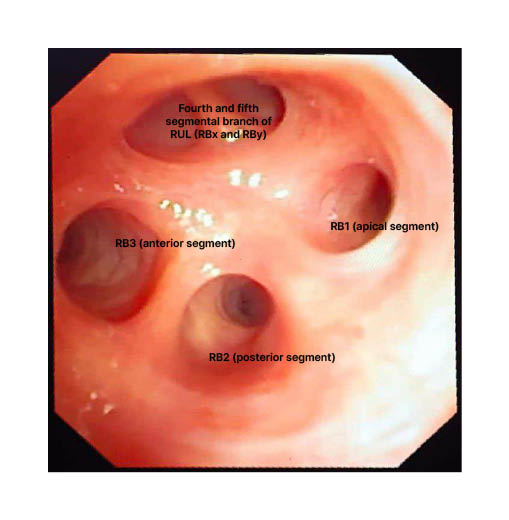
Figure 1: Flexible bronchoscopy showing five segmental divisions of the right upper lobe bronchus.
RB: right bronchus; RUL: right upper lobe.
DISCUSSION
Several models have been mentioned in the literature for pulmonary morphometry that were based on the concept of the pulmonary branch and airway generation to model geometry.5-9 The term right post-eparterial bronchus has been mentioned in the literature for any bronchus that emerges from the right bronchial tree at a level lower than the right upper lobe bronchus (eparterial bronchus).10
The difference in the anatomy of the airways is thought to result from a problem with lung formation, such as when too few lung buds form, or when they form at unusual locations. According to the research, tracheal bronchi and supernumerary superior segmental bronchi are the two most prevalent bronchial abnormalities, which are typically on the right side of airways.11
Traditionally, the apical segmental bronchi (B1), dorsal (B2), and ventral (B3) of the right upper lobar bronchus are separated. In the study conducted by Thiam et al.,12 only one instance exhibited quadrifurcation of the right upper lobe bronchus. There are numerous variations in bronchial segmentation that affect 43% of normal persons.13 These variants are predominately bifurcations, with a prevalence of 16.6–71.6% in the right upper lobe.13,14
Foster-Carter15 distinguished between supernumerary bronchus (the simultaneous presence of all segmental bronchi) and displaced bronchus (the location of a segmental bronchus distant from its theoretical origin). According to this, the authors’ case was a supernumerary bronchus.
In the authors’ present case, the radiological presentation, adding to this that the patient had a history of former bidi smoking and biomass fuel exposure, is suggestive of diagnosis of chronic obstructive pulmonary disease and old treated pulmonary Koch’s. However, the presence of ground-glass opacities and sub-pleural fibrotic bands raises the possibility of an additional diagnosis of lung cancer or tuberculosis, given the patient’s history of anti-tubercular treatment use and haemoptysis. The bronchoscopy revealed a rare anatomical variant of the right upper lobe bronchus with five branches. Although this finding may be incidental and unrelated to the patient’s presenting symptoms, it is, however, important to note the existence of such an anatomical variant, as it may have implications for diagnostic and therapeutic interventions in the future. The majority of these anatomical variations are asymptomatic and incidental, but there are few case reports and series in literature that suggest haemoptysis as a symptom related to tracheobronchial anatomical variation.16-18
In 0.1–2.0% of bronchoscopic examinations, a tracheal bronchus, sometimes known as a pig bronchus, is discovered; it almost always develops on the right.19 This variant describes a number of abnormal bronchial patterns, including classic pre-eparterial bronchus (the trachea’s misplaced right upper lobe apical segmental bronchus), classic tracheal bronchus (tracheal apical segmental bronchus with misplaced right upper lobe), and tracheal apical segmental bronchus that are extraneous. With an overall prevalence of 1–12%, other types previously described include auxiliary cardiac bronchus,20 ectopic, and accessory bronchus.21
The right upper lobe is considered as having the largest percentage of variants by most authors.21-23 The prevalence of right upper lobe variation in these studies varies from 1.2–54.0%. The prevalence of these variations varies widely across different studies, which may be due to factors such as differences in study populations and methods of classification. However, the right upper lobe variant with five segments spotted by the authors was unique, as it has never been described in the past, despite a tedious literature search. Right middle and lower lobe variants have also been described in literature.24
In a study, apart from the above-mentioned variants, a few other right upper lobe bronchus variants were described, including bipartite branching at the entrance, two segmental bronchus, and four segmental bronchus.25
The clinical significance of these variations is mainly related to their potential impact on diagnosis, treatment, and outcomes. In some cases, anatomical variations of the right upper lobe bronchus can lead to technical difficulties during diagnostic procedures, such as bronchoscopy or imaging studies. Furthermore, anatomical variations of the right upper lobe bronchus can impact the distribution of inhaled medications, and the development of atelectasis or aspiration. An understanding of these variations is, therefore, important for appropriate diagnosis and management of respiratory diseases. In some conditions, such as atelectasis or lobar pneumonia, recognising anatomical variations of the right upper lobe bronchus can be essential in determining the most appropriate therapeutic approach. They can also result in complications during surgery, particularly in cases of resection of the right upper lobe. Although variations in bronchial anatomy are a rare clinical entity and are usually asymptomatic, their recognition and correct diagnosis are eminent to know, as few entities may require clinical, endobronchial, and, in some instances, surgical interventions.
In conclusion, bronchoscopy is a valuable diagnostic tool to evaluate the bronchial tree and detect anatomical variations, such as the penta-segmental right upper lobe bronchus. Radiologists and clinicians should be aware of this anomaly to ensure appropriate management of pulmonary disorders, particularly in patients requiring bronchoscopy or surgical interventions. Newer techniques, including virtual, mixed, and augmented reality, are in development for studying the digital anatomy of the lungs and airways.27
Limitation of this case report is due to the rarity of the occurrence, and it is the first case at the authors’ institute with penta-lobe bronchus division finding of the right upper lobe. So, definite comment and implications on its clinical and surgical management is not possible.
The patient was admitted for investigations, and management, and was greatly relieved of her presenting complains of shortness of breath. She was discharged with medication advice, and is continuing follow-up in outpatient department, as per advice and her schedule. She was informed of the anatomical variation of her case, and informed consent was taken for reporting her case.
CONCLUSION
Overall, this case report highlights the importance of considering a wide range of differential diagnoses in patients with chronic respiratory symptoms, particularly in those with a history of smoking or biomass fuel exposure. Close attention to CT findings and bronchoscopy results, as well as knowledge of anatomical variants, can aid in accurate diagnosis and appropriate management. Further studies may be needed to investigate the prevalence and clinical significance of rare variants of the bronchial tree.






