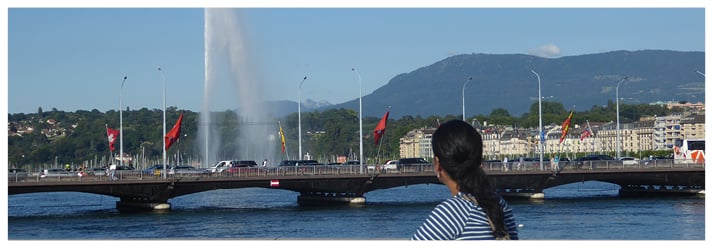
The diverse city of Geneva, Switzerland was the location for the 33rd Annual Meeting of The European Society of Human Reproduction and Embryology (ESHRE), which warmly welcomed senior scientists and clinicians from around Europe to attend this much anticipated meeting from 2nd–5th July. Known as both the ‘city of peace’ and Europe’s most international city, with >40% of its population originating from outside of Switzerland, Geneva also boasts spectacular views of Lake Geneva and the breath-taking Alps mountain range, as well as offering a rich and vibrant history, making it the perfect backdrop for this prestigious congress.
The 4-day meeting involved an open programme selected from >1,700 abstracts, of which the highest number came from China, for the first time in the congress’ history. Breaking yet another record, the number of abstracts submitted by females exceeded that by males, totalling 985 and 740, respectively. ESHRE Past Chairman, Dr Kersti Lundin, in her pre-congress statement in ‘Focus on Reproduction’, was proud to announce: “No other meeting in reproductive medicine can now command this sort of support year after year.” In our Congress Review section, we will bring you unmissable details and highlights from the 235 abstracts that were selected for oral presentation and a further 800 for poster presentation. As part of the social programme, attendees took a well-deserved break from congress by participating in ESHRE’s charity run on Monday 3rd July, which helped raise funds for patient groups throughout Europe including Fertility Europe, ESHRE’s partner patient organisation.
The high-quality scientific programme commenced with two keynote lectures. The first winning study was presented by world renowned clinical investigator, Prof Carlos Símon, and was based on his paper ‘Autologous cell therapy with CD133+ bone-marrow derived stem cells for refractory Asherman’s syndrome and endometrial atrophy: a pilot cohort study’. Presenting to one of the largest audiences in reproductive medicine, Prof Símon was followed by chemical pathologist Prof Dennis Lo for the second keynote presentation, providing the spectators with an update on non-invasive prenatal testing, which he argued will play a vital role in obstetric care. The meeting programme was packed full of topics of great importance to the discipline, including ovarian rejuvenation, germline gene editing, endocrine disruptors, cryopreservation, artificial gametes, and pregnancy failure. Of particular interest was the revelation of the much anticipated first results from ESHRE’s ESTEEM trial, a preimplantation genetic testing study of polar body analysis by array comparative genomic hybridisation (aCGH).
To bring this magnificent meeting to an end, newly appointed ESHRE Chairman Dr Roy Farquharson presented the awards and closing ceremony. João Pedro Alves Lopes (Sweden) was awarded the Basic Science Award for oral presentation; Heleen Zandstra (Netherlands) was awarded the Clinical Science Award for oral presentation; Ellen Casser (Germany) received the Basic Science Award for poster presentation; Paula Piomboni (Italy) was awarded the Clinical Science Award for poster presentation; Mina Popovic (Belgium) was given an educational travel grant to present her oral presentation at the annual meeting of the Fertility Society of Australia; Sarah Bailey (UK) was awarded the best oral presentation by a nurse; and Sofie Ellegiers (Belgium) was awarded the best oral or poster presentation made by a laboratory technician. In addition, Marc Germond (Switzerland) and Rob Norman (Australia) were appointed as the new ESHRE honorary members.
In the following review highlights, we will explore the very best of the pioneering research presented at this year’s ESHRE meeting, providing a convenient overview for those of you who were unable to attend, or a welcome refresher for those who would like to re-visit the fascinating meeting. We hope you will enjoy reading our highlights and we look forward to seeing many of you at next year’s ESHRE meeting, 1st–4th July, in the home of Gaudí architecture, Barcelona, Spain.

Artificial Intelligence Improves Assessment of Embryo Quality
ERRORS in the morphological assessment of embryo quality could be improved by advances in artificial intelligence, according to a ESHRE press release dated 4th July 2017.
Embryo quality is considered the main determinant of implantation and pregnancy in in vitro fertilisation (IVF). Morphology is used to measure embryo quality; however, a visual morphological grading can lead to variation. Recently, morphological grading has become more accurate with the introduction of time- lapse imaging. Unfortunately, many embryos graded as ‘good quality’ still fail to implant in the uterus and lead to pregnancy. It is thought that this is due to chromosomal abnormalities, which are not detected by morphological assessment.
A recent study from São Paulo State University, São Paulo, Brazil, has analysed images taken from the development of 482 7-day-old bovine embryos, which were used to ‘train’ an artificial intelligence system. Thirty-six assessment variables were identified during the analysis, 24 of which formed the input of the artificial network architecture. By using mathematical variables derived from time-lapse images of embryo development, an algorithm can classify images of an embryo’s development automatically, removing the human variable from morphological assessment. During the initial set-up phase, ‘serious errors’ occurred in only 6% of the assessments and, overall, the artificial intelligence system had a 76% accuracy.
By increasing the objectivity and repeatability in embryo assessment, accuracy of diagnosing embryo viability can be improved. Clinicians can use this artificial intelligence to customise their treatment strategies and better predict a patient’s chance of pregnancy.
Investigator Prof Jose Celso Rocha, São Paulo State University, suggested that embryo assessment led by artificial intelligence could be ready for routine clinical use within the next 2 years, at least as a controlled and test version; however, the extent to which it will improve embryo grading, and thus outcome in IVF, will depend on how thoroughly the system is ‘trained’ and how wide the sampling of embryo images is in that training.
Quantity and Quality Are Both Important for IVF Success
A HIGHER number of eggs retrieved during an in vitro fertilisation (IVF) treatment cycle is associated with more chromosomally normal embryos available for transfer. Results from the Australian study, conducted by Dr Christos Venetis, University of New South Wales, Sydney, New South Wales, Australia, and IVF Australia, were presented at this year’s ESHRE conference and summarised in a ESHRE press release dated 3rd July 2017.
The study assessed the number of chromosomally normal (euploid) embryos identified during preimplantation genetic screening in 724 cycles at three IVF centres. The euploid embryos were then correlated with the number of oocytes received during that treatment cycle. Results showed that the number of euploid embryos identified per cycle was negatively associated with female age. For one euploid embryo to be produced, a 34-year-old woman would need to produce five oocytes, whilst a 38-year-old would need 10; as for two euploid embryos, 14 and 24 would be needed, respectively. It was also shown that the number of oocytes received was positively associated with the number of euploid embryos generated; the higher the number of oocytes, the higher the number of euploid embryos produced. Previous research had indicated live birth rates were also correlated to the number of oocytes received.
Euploid embryos are known to have a high probability of implantation (50–60%) and low probability of miscarriage (6%). This study suggests, according to Dr Venetis, University of New South Wales, that a higher number of oocytes leads to a higher number of euploid embryos available for transfer which “clearly correlated with the cumulative chance of a pregnancy after a single stimulated cycle.” Simply, the more oocytes collected during a single round of IVF treatment, the higher the chance of euploid embryos developing, leading to an increased chance of healthy live births.
There is no universal oocyte number to collect, as other parameters need to be taken into account, including specific patient’s wishes. Dr Venetis mentioned that aiming for a high number of eggs (>15) can increase the risk of ovarian hyperstimulation syndrome (OHSS) and potential complications. New stimulation protocols, however, greatly reduce the risk of OHSS, which may allow the yield from a single stimulation to be much greater.

Mosaic Embryos Can Lead to a Healthy Pregnancy
IMPLANTING mosaic embryos during in vitro fertilisation (IVF) can result in a healthy pregnancy. This is according to the results of a new study by Dr Francesco Fiorentino, GENOMA Laboratory, Rome, Italy, and colleagues, reported in a ESHRE press release dated 4th July 2017. Mosaic embryos are those whose cells have ≥2 cell lineages that are genetically distinct. Generally, one cell lineage will have a normal chromosome composition and the other will have a chromosome abnormality.
During IVF, preimplantation genetic testing for aneuploidy is typically used to discern euploid (chromosomally normal) embryos and thereby boost the likelihood of a successful IVF outcome. Until recently, mosaic embryos were not commonly utilised in IVF, as it was believed their use would not result in a successful procedure. However, a previous study by Dr Fiorentino’s group had suggested that mosaic embryos could lead to a healthy pregnancy.
Building on this finding, the study involved 73 women who did not have any euploid embryos for transfer but did have mosaic embryos. Researchers classified the mosaic embryos into two categories: high aneuploidy (≥50%) and low aneuploidy (<50%). It was found that transfers of embryos in the low aneuploidy category led to a live birth rate of 39.5% and a miscarriage rate of 7.0%. This was in comparison to a live birth rate of 16.7% and a miscarriage rate of 10.0% in the high aneuploidy category. This finding led Dr Fiorentino to suggest that: “Priority for transfer should be given to mosaic embryos with low levels of aneuploidy.”
Furthermore, the researchers concluded that their results demonstrated mosaic embryos should now be considered a distinct category in regard to likelihood of a successful IVF procedure. Dr Fiorentino explained: “Euploid embryos have a higher implantation potential than mosaic embryos, and because of this we suggest that mosaic embryos should only be transferred in women with no euploid embryos available.”
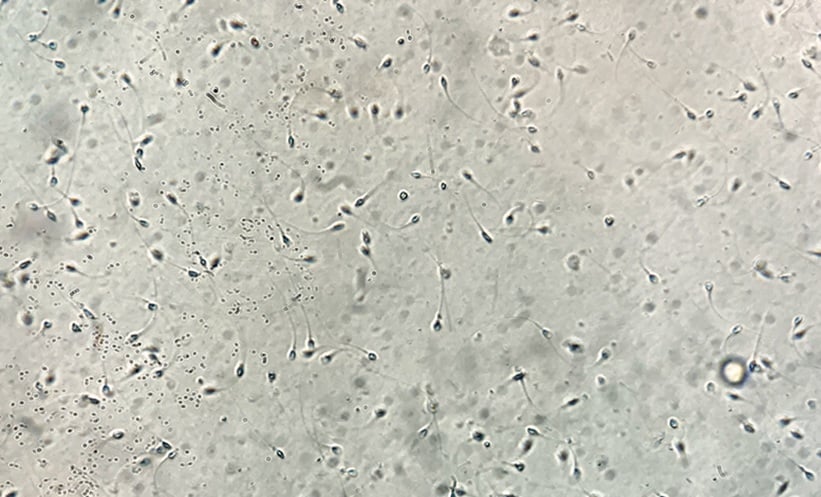
Male Partner Age Affects IVF Delivery Rates
INCREASING male age was the subject of a recent study which investigated the correlation between the age of a male partner and live birth rates in couples using in vitro fertilisation (IVF) to conceive. Aside from a handful of studies into natural conception and the impact of male partner age, little was known about this subject until recently, because female age is such a dominant factor in successful conception.
In a ESHRE press release dated 3rd July 2017, Dr Laura Dodge, Harvard Medical School, Boston, Massachusetts, USA, explained: “Generally, we saw no significant decline in cumulative live birth when women had a male partner the same age or younger. However, women aged 35–40 did significantly benefit from having a male partner who is under age 30, in that they see a nearly 30% relative improvement in cumulative incidence of live birth when compared to women whose partner is 30–35, from 54% to 70%.”
The team analysed the IVF cycles that had been completed between 2000 and 2014 at a large IVF centre in Boston. This amounted to nearly 19,000 cycles for 7,753 couples, with female partners grouped according to the following age ranges: <30, 30–35, 35–40, and 40–42 years of age. Male partners were also grouped into these age bands, but there was an additional group for >42 years. They found that couples where the female was in the 40–42-year age range had the lowest cumulative live birth rate, and in these instances the age of the male partner had no impact on the success of the cycle. This confirms the impact of female age on success rates of IVF. Increasing male age, however, was shown to have a negative effect on the success rates when the female was in other age groups; for example, if the female partner was aged <30 years, a male partner aged 40–42 years was associated with a 46% lower cumulative birth rate than if the male partner was aged 30–35 years. If female partners were aged 35–40 years, a younger male partner was more likely to produce a higher live birth rate.
Clomiphene Citrate to Become the Drug of Choice for Ovarian Stimulation Before Intrauterine Insemination
A NON-HORMONAL fertility drug, in addition to being much cheaper, has been shown to be just as effective as hormones for ovarian stimulation before intrauterine insemination (IUI) in a study reported on in a ESHRE press release dated 3rd July 2017. According to the researchers from the AMC Centre for Reproductive Medicine, Amsterdam, Netherlands, these results will make this the drug of choice for IUI in couples with unexplained and mild male infertility.
The ovarian stimulation prior to IUI method is associated with an increased risk of multiple pregnancy, and therefore there has been some debate as to whether it should be performed with a course of routinely used injections of follicle stimulating hormone (FSH) or with a shorter course of the non-hormonal drug clomiphene citrate (CC).
This study compared the two options in couples with unexplained or mild male infertility in 24 fertility centres in the Netherlands, randomising a cohort of women (N=738), to IUI with FSH (n=369) and to IUI with clomiphene (n=369). Of the patients studied, 113 (31%) and 97 (26%) had an ongoing pregnancy following IUI-FSH and IUI-CC, respectively. There were five (1%) cases of multiple pregnancies in the IUI-FSH cohort, and eight (2%) in the IUI-CC group. These differences were statistically insignificant.
Additionally, ovarian stimulation with CC was much cheaper financially than with FSH, with the latter estimated as costing just €5 per patient after 5 days of daily tablets. This compared to an estimated €200 per patient for those who received FSH injections for a mean duration of 8 days.
“We showed that IUI stimulated with FSH is not superior to IUI and clomiphene in terms of ongoing pregnancies, live births, and time to pregnancy,” commented investigator Dr Noor Danhof, AMC Centre for Reproductive Medicine. “We also found a comparable low multiple pregnancy rate between IUI-FSH and IUI-CC, and these are now the reasons why we recommend using the least expensive stimulation agent.”
Pregnancy in Cancer Survivors Quantified for the First Time
FEMALE survivors of cancer are 38% less likely to achieve a pregnancy than women who have never been subject to the disease, suggests a study performed by the Medical Research Council Centre for Reproductive Health, Queen’s Medical Research Institute, University of Edinburgh, Edinburgh, UK, presented at the ESHRE annual meeting, 2017, and described in a ESHRE press release dated 3rd July 2017.
The study noted the incidents of pregnancy in 23,201 cancer survivors ≤39 years of age, who were diagnosed in Scotland between 1981 and 2012, and found that only 20.6% of them achieved pregnancy, compared to 38.7% of the control group. This chance of pregnancy was reduced in all age groups and was particularly low in those women with cervical cancer, breast cancer, and leukaemia. “The major impact of pregnancy after some common cancers highlights the need for enhanced strategies to preserve fertility in girls and young women,” said Prof Richard Anderson, University of Edinburgh.
Another notable discovery was that those diagnosed with cancer later in the study (2005–2012) had higher rates of pregnancy than those diagnosed earlier (1981–88), indicating that the impact of some cancer treatments on fertility rates has reduced.
Prof Anderson was quick to point out the limitations of the study, not least that some women may have simply chosen not to have a pregnancy, explaining: “While these results do show an expected reduction in the chance of pregnancy after chemotherapy and radiotherapy, having a pregnancy after cancer does involve a range of complex issues that we cannot address in this study.”
Researchers are hopeful that these data will help clinicians to advise their patients more accurately concerning their future chances of pregnancy, particularly with respect to fertility preservation methods, such as oocyte and embryo freezing. “Even for patients considered at low risk of infertility as a result of treatment, a fertility discussion is recommended before treatment begins,” concluded Prof Anderson.
Single-Mother-By-Choice Children Do Just as Well
CHILDREN in single-mother-by-choice families do as well as those in heterosexual two-parent families, according to a ESHRE press release dated 5th July 2017. Fertility treatment for single women is now an increasingly popular choice for women who wish to become pregnant without a partner, but some specialists have raised concerns about the wellbeing and development of the resulting children. A study from the Centre of Expertise on Gender Dysphoria, VU University Medical Centre, Amsterdam, Netherlands, found no differences in terms of parent-child relationship or child development, and discovered that single-mothers-by-choice had a greater social support network.
The study compared 69 single-mothers-by-choice (who had knowingly chosen to raise their children alone) and 59 mothers from heterosexual two-parent families with a child between 1.5 and 6 years of age. Using three validated questionnaires, parent-child relationships, mothers’ social support networks, and children’s wellbeing were compared. The study found that, for parent stress or emotional involvement there were no significant differences between family types; single-mothers-by-choice showed significantly higher scores on the social support they received; and there were no significant differences in the children’s wellbeing between both family types. The study reported that children growing up with single-mothers-by-choice seemed to enjoy a similar parent-child relationship to those in heterosexual two-parent families.
Ms Mathilde Brewaeys, study investigator from the Centre of Expertise on Gender Dysphoria of the VU University Medical Centre, said: “The assumption that growing up in a family without a father is not good for the child is based mainly on research into children whose parents are divorced and who thus have experienced parental conflict. However, it seems likely that any negative influence on child development depends more on a troubled parent-child relationship and not on the absence of a father.”
The study also found that single-mothers-by-choice and their children benefit from a good social support network and that this should be emphasised in the counselling of women who want to have a child without a partner.

Use of Assisted Reproductive Technology in Europe
GLOBAL need for advanced fertility treatments are not being met by the majority of European countries, according to a presentation displayed in a ESHRE press release dated 4th July 2017. This study covered 707,171 treatment cycles performed in 2014 and the subsequent 146,232 babies born, making this the largest, most accurate snapshot of assisted reproductive technology (ART) in Europe. Spain was found to be leading in ART activity, performing 109,275 treatment cycles in 2014, followed by Russia (94,985) and, former leaders, France (90,434); the UK performed 61,000 treatments in 2013. The total number of treatment cycles included in vitro fertilisation (IVF), intracytoplasmic sperm injection (ICSI), egg donation, and intrauterine insemination.
Numerous findings were presented, with ICSI being continually favoured over IVF in clinics, with 336,123 and 123,809 procedures performed, respectively, despite pregnancy rates, per embryo transfer, being higher with IVF (34.6%) than ICSI (33.1%). ICSI was first developed in the 1990s to allow infertile men to conceive, but now the procedure is predominantly used for occasions with no male partners.
Throughout Europe, pregnancy rates have stabilised for both IVF and ICSI, 35% and 33%, respectively, but pregnancies resulting from egg donation have continued to rise, currently at ˜50%. However, these statistics do fluctuate between countries. It was also acknowledged that pregnancy rates from blastocyst transfers are continuously higher than Day 3 transfers, across all processes. Rates from frozen donor eggs (49%) were found to be very similar to fresh donor eggs (51%), but higher than frozen embryos. Twin pregnancy rates, once common in IVF, are continuing to fall, reaching ˜17% in 2014. Dr Calhaz-Jorge, Chairman, European IVF Monitoring Consortium for ESHRE summarised: “The rate of multiple pregnancy continues its slow but steady decline. Success rates seem to have stabilised.”
Unfortunately, availability of ART remains very uneven across Europe; a study calculated a global need for ART at ~1,500 cycles per million population per year. Dr Calhaz-Jorge commented: “Only a minority of European countries meet this need.”
Positive Trials Towards Personalised Medicine in Fertility Patients
ANALYSES of two Phase III clinical trials (ESTHER-1 and ESTHER-2) have demonstrated that treatment with Rekovelle® (follitropin delta) produces similar live birth rates to conventional follitropin alfa treatment. The analysis, performed by Ferring Pharmaceuticals, Saint-Prex, Switzerland and presented at the ESHRE Annual Meeting 2017, showed the cumulative live birth rate following in vitro fertilisation to be 43.9% with follitropin delta; just 0.6% lower than with follitropin alfa. Ongoing pregnancy rates were equally similar (45.1% and 45.7%, respectively). “These new Rekovelle analyses add further evidence for a personalised approach to fertility treatment for patients,” said Per Falk, Executive Vice President and Chief Scientific Officer, Ferring Pharmaceuticals.
A separate analysis of the safety profile of the drug was also performed. Using data from the ESTHER-1 trial, researchers evaluated ongoing pregnancy rates, early ovarian hyperstimulation syndrome (OHSS), and preventative interventions for early OHSS in women with varying anti-Müllerian hormone (AMH) levels. In women with high AMH (≥35 pmol/L) results showed a lower incidence of early OHSS for follitropin delta in comparison to conventional follitropin alfa dosing (4.7% versus 11.9%, respectively). The analysis also revealed a significant improvement in the amount of patients requiring preventative interventions for early OHSS; 4.7% for follitropin delta treatment versus 23.8% for follitropin alfa. It was notable that patients’ ongoing pregnancy rate was sustained.
Researchers were quick to note that the ESTHER trials were not powered for this analysis, thus further study will be required before the efficacy of the drug can be validated. Nonetheless, researchers are confident that these analyses represent a promising step towards personalised fertility treatment. “Rekovelle’s individualised dosing regimen, based on a patient’s AMH level and body weight, provides clinicians with a consistent, evidence-based approach to personalising treatment for their patients,” concluded Per Falk.