
Abstract
A young male presented with chest pain after blunt chest wall trauma. Immediate CT coronary angiography demonstrated a spiral dissection of the right coronary artery. CT fractional flow reserve confirmed modest flow limitation so the patient was treated medically. At follow-up CT the vessel had healed and CT fractional flow reserve had normalised.
BACKGROUND
The incidence of traumatic coronary artery dissection is rare, but it can be life-threatening. It is underdiagnosed because the chest pain following a physical injury is often attributed to the musculoskeletal bruising resulting from the impact itself. In some cases, ECG helps to make a diagnosis of myocardial infarction but in the absence of ECG changes, a high index of suspicion is required to pursue cardiac-specific investigations such as high-sensitivity troponin.
This paper presents a young male with chest trauma during martial arts practice presenting with right coronary artery (RCA) dissection, diagnosed on immediate CT coronary angiography (CTCA). Using the novel technique of CT fractional flow reserve (FFRCT), this was shown to be only minimally flow-limiting and he was managed medically with antiplatelet agents rather than stenting. A follow-up CTCA at 2 months confirmed the complete healing of the artery with normal flow on FFRCT.
CASE
A 30-year-old male developed sudden-onset chest heaviness, radiating to his left shoulder, after being punched in the chest during a competitive karate match. He presented to hospital with excruciating chest pain. Clinical examination and a chest X-ray were normal. ECG confirmed early repolarisation changes but was otherwise normal.
Serial troponins were, retrospectively, elevated at 99 and 199 at 3 and 6 hours post-event, where the normal range is <15; the rest of the blood tests were normal. An initial diagnosis of probable acute coronary syndrome was made, and the patient was treated with dual antiplatelet, anticoagulant, and statin therapies as per the local protocol. Given the potential delay in interhospital transfer for invasive cardiac catheterisation at a nearby centre, immediate CTCA was performed locally. The CTCA revealed a spiral filling defect (Figure 1) in the proximal RCA, highly suggestive of spiral dissection. Given the uncertainty about the flow, noninvasive assessment of coronary physiology using the new technique of FFRCT was performed. This confirmed a slightly reduced FFRCT of the proximal lesion of the RCA at 0.88 (Figure 2). Generally, stents are not inserted unless the FFRCT is <0.80.
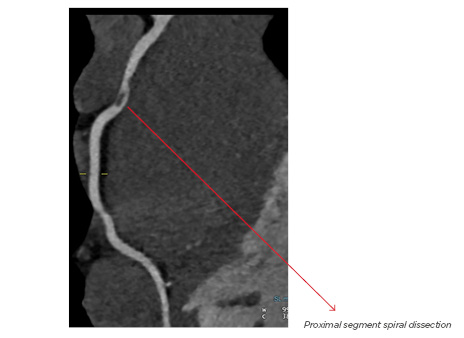
Figure 1: Index scan of reconstructed right coronary artery from CT coronary angiography.
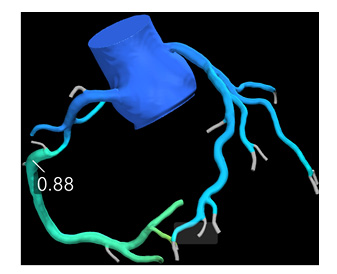
Figure 2: CT fractional flow reserve on admission.
After discussion at a multidisciplinary meeting, it was deemed appropriate to perform the traditional ‘gold standard’ invasive coronary angiogram to confirm the diagnosis of coronary dissection. Invasive coronary angiography confirmed spiral dissection of the proximal RCA with normal blood flow distally, and intravascular ultrasound confirmed this was due to a limited spiral dissection. Transthoracic echocardiography confirmed normal left ventricular systolic function without any evidence of wall motion abnormality.
The final diagnosis of coronary artery dissection secondary to the blunt chest wall trauma was reached and managed medically with dual antiplatelet and statin therapies. A follow-up CTCA 8 weeks later confirmed the RCA dissection had healed anatomically (Figure 3) and repeat FFRCT was increased with now completely normal flow. There was no coronary artery disease visible, so the statin was stopped and dual antiplatelet therapy reduced to aspirin alone.
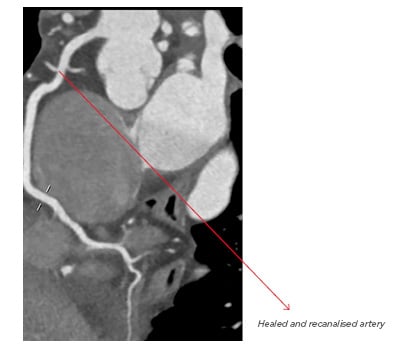
Figure 3: Follow-up study of reconstructed right coronary artery from CT coronary angiography.
CONCLUSION
Coronary artery dissection secondary to blunt trauma is rare but can lead to myocardial infarction1-3 and can be fatal.4 The involvement of the RCA is extremely unusual, with very few cases having been reported in the literature.5,6
In this case, the diagnosis was made on immediate CTCA.7 Coronary dissection without any associated atherosclerotic plaque disease on CTCA, and lack of significant impairment to coronary blood flow on the novel technique of FFRCT, allowed for conservative management as opposed to stent implantation.8 This has not previously been reported and may allow many patients to have rapid non-invasive diagnosis without the need for invasive coronary angiography. In this case, invasive coronary angiography was performed to confirm the diagnosis, but it added nothing to the CTCA information and could potentially have extended the dissection. This case demonstrates that utilisation of noninvasive CTCA and FFRCT in acute situations could help direct appropriate management of the patient. This case also demonstrated the utilisation of noninvasive CTCA for follow-up to ensure the complete recanalisation of the artery.
LEARNING POINTS
- Blunt chest wall injury during sport can cause traumatic coronary dissection and should be considered in patients with severe chest pain.
- CTCA and FFRCT can be utilised as first-line investigations in suspected traumatic coronary artery dissection for both anatomical diagnosis and to confirm the physiological significance.
- Follow-up CTCA should be considered to ensure the complete recanalisation of the artery.




