Abstract
This study examines the relationship between vaccination and inflation in battling the COVID-19 pandemic across nations. Data from 85 countries worldwide were collected from the Trading Economics (New York City, USA) website during the COVID-19 pandemic. First, a new theoretical model was proposed based on the economic and healthcare literature; then, a binary variable, inflation/vaccination% was developed according to the proposed theoretical model. The relationship between inflation/vaccination% and macroeconomic factors was examined using logistic regression. After that, the countries were ranked by minimising the inflation/vaccination% rate that measures a country’s efficiency in fighting the COVID-19 pandemic, thereby permitting governments to compare the performance of different countries. The findings show that a country with a higher gross domestic product growth rate and competitiveness index during the COVID-19 pandemic has a lower inflation/vaccination% ratio. The results of this study provide strong evidence that countries should mitigate a pandemic’s economic impact by managing vaccination programmes to control global inflation.
Key Points
1. This research shows that managing vaccination programmes during a pandemic can help mitigate the impacts of rising global inflation. The findings are highly relevant for future pandemics, as this approach can help effectively plan for the pandemic, reducing the overall impact on society.
2. The research describes the interrelationship between the vaccination rate and global inflation during the COVID-19 crisis. The findings rank countries based on their economic and health sectors battling the COVID-19 pandemic and provide implications for future pandemics.
3. An important message from this research for clinicians is demonstrating how to help their patients resume their normal lives following a pandemic. Healthcare professionals can be key players in accelerating the vaccination process, helping to reduce the long-term impacts of this crisis. To achieve this goal, it is essential that they take proactive action and work together to make it happen.
INTRODUCTION
In late 2019, a highly contagious virus from the family of severe acute respiratory syndromes originated from Wuhan, China, and spread around the world in 2020.1,2 This experience suggested the need to examine how countries can mitigate the economic effects of pandemics.
The World Health Organization (WHO) declared the COVID-19 pandemic on 11th March 2020. This disease is contagious and is caused by severe acute respiratory syndrome coronavirus 2.3 As of 26th July 2023, around 768 million cases and 6.95 million deaths were reported worldwide.3 Despite scientists having developed several vaccines, the number of COVID-19 infections and deaths is still increasing, with a negative acceleration slope worldwide.
Some scientists believe that the COVID-19 pandemic is one of the worst pandemics in the world,4 and some scientists have predicted a K-, L-, U-, or V-shaped economic recovery following the pandemic, depending on the amount of time needed to return to normalcy.5 However, it is still hard to find an absolute recovery model with the emergence of new variants of the virus, even after vaccine development.
One of the negative impacts of the COVID-19 pandemic is global inflation, which was caused by the disruption of the global supply.6-8 Inflation is one of the critical macroeconomic factors for households, which could cause a range of decisions that affect a society’s savings, borrowing, and consumption during the COVID-19 pandemic.6,7 Therefore, global inflation control requires that businesses and their supply chains practise overcoming lingering COVID-19 pandemic issues. To achieve this goal, the healthcare system can play a major role and help people get vaccinated faster, which will help restore normal life before the pandemic.
Almost 1 year after the start of the COVID-19 pandemic, health service scientists developed various types of vaccines (e.g., mRNA, inactivated virus, or non-replicating virus vector).9-12 However, people have not been vaccinated at the rates governments anticipated.13 For example, as of 2nd December 2022, only 69.2% of the world’s population, and 25.9% of low-income countries, have been vaccinated with one dose of COVID-19 vaccines.14
Deiana et al.15 and Li et al.16 indicated that reluctance to get vaccinated was partially due to a belief that the new vaccines were not adequately planned. Machingaidze and Wiysonge17 and Shrestha et al.18 reported that side effects, safety, competence, and effectiveness of the vaccines were yet to be clarified. Khatiwada et al.19 and Machingaidze and Wiysonge17 suggested that vaccine hesitancy could also be attributed to rapid vaccine development and media misinformation. Nemat et al.20 and Adebisi et al.21 suggested that people were concerned about the reliability of the vaccines in some countries, or that they may possess natural immunity against the COVID-19 virus. Armantier et al.6 and Detmers et al.7 found that hesitancy to get vaccinated and return to the normal job situation exacerbated supply chain disruption issues, which may be a cause of higher global inflation.
This paper seeks to add to the existing literature by developing a theory through a binary variable connecting economic factor, inflation, with healthcare variable, vaccine rates, during the COVID-19 pandemic. It then examines the interrelationships between macroeconomic factors and inflation/vaccination%, as well as ranking countries’ efficiency in combating the pandemic based on their health-economic factors.
INFLATION-VACCINE THEORY
The COVID-19 pandemic caused problems for both public and private sectors.22-25 Several sectors (e.g., households, businesses, and governments) have been affected by the COVID-19 pandemic. McKibbin and Fernando26 and Ahangar and Kim27 examined the effects of the pandemic on different macroeconomic sectors (i.e., labour supply, equity risk premium, consumption demand, government expenditure, production, and gross domestic product [GDP]). They found that the consumption demand shock on GDP was more influential than the other shocks in households’ lives. The inflation rate is one of the critical macroeconomic factors influencing households that may cause a consumption demand shock. Studies by Crump et al.,28 D’Acunto et al.,29 Detmers et al.,7 and Candia et al.30 have demonstrated a relationship between households’ economic behaviour and their expectations of future inflation during the COVID-19 pandemic. Wulandhari et al.25 argued that COVID-19 caused a supply shock, which could result in a higher inflation rate for households. Bobeica and Hartwig31 asserted that, in early 2021, the primary cause of high inflation was the increase in supply side and commodity prices. Moreover, Armantier et al.,6 Detmers et al.,7 and Gautier et al.8 suggested that both supply and demand shocks due to COVID-19 and the lockdown could be the reason for high inflation.
Various plans were implemented by governments, and particularly healthcare systems, during the COVID-19 outbreak, such as mandates for lockdowns to control disease’s spread.32,33 These efforts can reduce the number of deaths caused by the disease but can also lead to social and political disruption and economic slowdown. Harland et al.,34 in their study about healthcare during the COVID-19 pandemic, showed that the development and implementation of plans in healthcare systems that can withstand future emergencies depend upon understanding their capabilities and the motivation to use them during a pandemic. Finkenstadt and Handfield35 highlighted that the emergence of a new virus during the pandemic led to a significant vaccine shortage, and the lessons can improve the planning for healthcare and future pandemic vaccines. The idea of a social vaccine suggests that popular mobilisation and advocacy can be encouraged to change social and economic structural conditions that make people and communities vulnerable to disease.36
During the COVID-19 pandemic, Dorn et al.37 developed a new theory examining the relationship between public healthcare and economic systems. They demonstrated that balancing interests between public health and the economy is essential during the pandemic. The monetary theory of inflation38 declares that the growth of cash flow or money supply is the primary cause of inflation. Thus, injecting cash flow (e.g., subsidy or stimulus check) into the market can lead to faster inflation in nations. In economics, disposable personal income, defined as money households retain after paying taxes or receiving government assistance (e.g., stimulus checks), is critical in understanding a society’s economic security and inflationary challenges.39 For instance, Jorda et al.39 found that government stimulus checks distributed to households during the pandemic contributed to a higher inflation rate in the USA. Additionally, Barnichon et al.40 and Bianchi et al.41 have conducted research, showing the effects of COVID-19 pandemic on inflation.
The healthcare industry represents a considerable portion of economic and social activities worldwide, with countries spending over 8% of GDP on healthcare.42 Employee commitment and control theories propose that employee initiatives are critical to patient safety.43 As such, healthcare plays a vital role in economics, making the availability of effective COVID-19 vaccines for the public at high speed. To this end, it is optimal to start the downstream task concurrently in cyclical projects.44 In a study, Shahmanzari et al.33 showed that the structure of containment measures strongly relates to critical economic and disease parameters, such as recovery rate, containment capacity, and infection rate. Bjurling-Sjöberg et al.45 developed a practical theory of resilient performance during a pandemic, highlighting the vital role of working conditions and patient safety during a COVID-19 pandemic. In addition, Sarabia et al.46 showed that a higher annual expenditure could be related to a lower incidence of COVID-19 in the health system.
Therefore, this study develops a theory and proposes an interrelationship between inflation and vaccination using inflation/vaccination% ratio and other macroeconomic factors to help countries control global inflation appropriately. Vaccinating people as soon as possible may reduce the need for stimulus income, help the economy retain jobs, and contribute to business health. The rationale suggests that inflation and the vaccination rate of people are related to each other, and if both are improved, the ratio of inflation/vaccination% would be smaller. However, to achieve this goal, some key macroeconomic factors must be improved along with the vaccination rate.
RESEARCH THEORETICAL MODEL
After reviewing the literature and synthesising economic and pandemic theories, the authors theorised that global inflation in a pandemic can be related to a nation’s healthcare system through other macroeconomic factors. To test this interrelationship between vaccination and global inflation rates, the authors constructed a theoretical model and analysed it using various macroeconomic variables across multiple market sectors. Thus, their theoretical model can be seen in Figure 1.
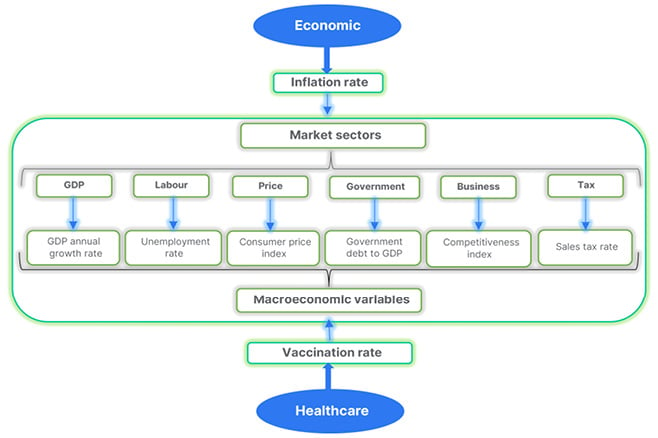
Figure 1: Theoretical model of inflation/vaccine ratio in this study.
GDP: gross domestic product.
This theoretical model indicates no direct relationship between the inflation rate and vaccination rate; however, the diagram indicates an interrelationship between this economic and health factor through other macroeconomic factors. The authors examined the direct and interrelation effects to answer the following research questions.
Research Questions
The important research questions that provide insight and recommendations to mitigate the economic effects of a pandemic were:
- Is there any interrelationship between the vaccination rate and global inflation during the COVID-19 pandemic?
- How can countries mitigate a pandemic’s impact by managing vaccination programmes to control global inflation?
- How can countries be ranked based on their economic and health sectors in battling the COVID-19 pandemic?
DATA AND METHODOLOGY
Data from 85 countries worldwide collected from the Trading Economics (New York City, USA) website47 were used for this study, which focused on macroeconomic variables relevant to the COVID-19 pandemic. In the initial step, the data of more nations, including 115 countries, were selected. After that, a nation with missing values was removed from the list. For some political and monetary sanctions, the authors short-listed 95 countries whose economic fluctuations have an economic base. Then ten countries were removed from the list based on the Box–Tidwell test, which checks the linearity between the explanatory factors and their natural log in the model. In the end, 85 countries were selected, for which the data was available and public, and there were no outliers or political/financial sanctions on their different sectors. Therefore, to ensure that the models were valid, various combinations of data preparation and tests were employed. High correlation variables were excluded, and no missing values were present. Furthermore, countries with extreme observations coming from a political rather than economic base were excluded.
First, the relationship between inflation/vaccination% and macroeconomic factors is examined using logistic regression. After that, the data envelopment analysis (DEA) was applied to measure a country’s efficiency in fighting the COVID-19 pandemic, thereby permitting them to compare the performance of different countries. Given the focus of the analysis on the inflation-vaccine ratio, a constant return to scale two-stage output-oriented DEA model was developed. The selection of input and output variables was based on the most influential variables identified in the logistic regression stage.
Dependent Variable
The dependent variable was the inflation/vaccination%, with the numerator being the inflation rate in December 2021 and the denominator being the total number of vaccinated individuals per 100 people in December 2021. This is a newly developed factor related to healthcare during the COVID-19 pandemic.
In this study, the authors used the median value of this fraction as a point for data segmentation. Any value lower than the median was labelled as ‘low’, and any value higher than the middle point was labelled as ‘high’. Each country had a specific value for inflation and vaccination rates, making their ratio unique. The authors ordered the numerical values from the largest to the smallest and divided them into two equal samples by determining the median value. This procedure produced extreme polar segmentation,48 which requires ordering of the observations of a variable. Then, the data was parsed into two data subsets that each contained half the values to maximise variance within the inflation/vaccination% variable.
Explanatory Variables
Previous studies have explored the various solutions for developing nations’ health related to the COVID-19 pandemic. These findings were broken down into economic and health factors, with nations’ economic health during the pandemic being measured using a set of economic indicators commonly reported by nations. Explanatory variables in this study have a ratio-level measurement scale, and they are selected from different sectors and their derivatives in the market (i.e., GDP, labour, price, government, business, and tax) to ensure that all aspects of a household affected by the COVID-19 pandemic shock are captured in the analysis.26,27
The variables selected for this study were the GDP annual growth rate from the GDP section, which shows a nation’s GDP change at market prices during the COVID-19 pandemic; the unemployment rate from the labour category, representing a portion of the labour force without a job but who are actively searching for a job during the pandemic; the consumer price index from price categories, which indicates an average change in prices paid by a household for goods and services during the COVID-19 pandemic; the government debt to GDP from the government section, to show a nation’s public debt to its GDP and a country’s ability to pay back its loans after the pandemic; the competitiveness index from the business section, to show a country’s productivity level during the pandemic; and the sales tax rate from the tax category, to show government aid in terms of subsiding during COVID-19. Additionally, the COVID-19 vaccination rate over time was chosen from the health side to indicate a nation’s health plan in batting against the COVID-19 pandemic.
RESULTS
Correlation Analysis
The authors examined the correlation between the explanatory variables to avoid selecting variables with a high correlation that would result in multicollinearity.49
Table 1 presents the correlation matrix of all regressors, as well as mean and standard deviation. Results demonstrate that correlations between independent variables are relatively low. Additionally, a mean variance inflation factor of 1.16 indicates that multicollinearity was not an issue in this study. Subsequently, a pair correlation plot analysis was conducted to graphically visualise correlations between each pair of variables.
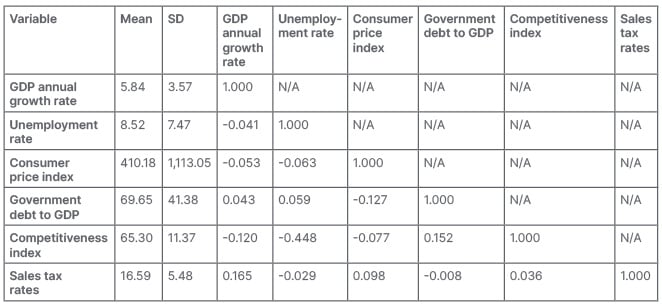
Table 1: Correlation matrix of macroeconomic explanatory variables in this study.
GDP: gross domestic product; N/A: not applicable; SD: standard deviation.
Logistic Regression Analysis
The authors performed logistic regression to examine the relationships between the binary variable, inflation/vaccination%, and the macroeconomic regressors. Table 2 shows the results from the logit model analysis, which models the probability of the ratio inflation/vaccination% falling below the central value, referred to as low. The likelihood ratio test (χ2: 105.15; p<0.001; pseudo-R2: 89.67%) supports that the overall model is significant at the 1% level.
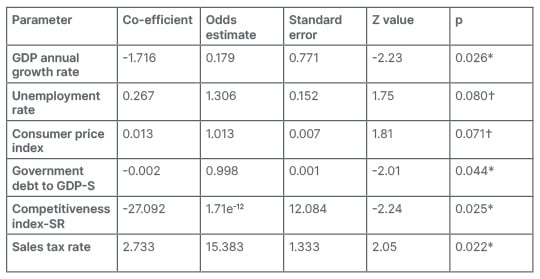
Table 2: A logit model analysis of maximum likelihood estimates for the variables in this study.
*Significant at p<0.05.
†Significant at p<0.10.
Sample size is 85. Government debt to GDP-S is the square of variable government debt to GDP, and competitiveness index-SR is the SR of the variable competitiveness index.
GDP: gross domestic product; GDP-S: square of the government debt to gross domestic product;
SR: square root.
Table 2 presents the estimated parameters, p values of independent variables, and the significant macroeconomic variables at 10% and 5% statistical levels. The intercept was also found to be statistically significant in this model. The odds estimates represent the log odds of the outcome for a one unit increase in predictor variables. According to the coefficients and odds estimates, the first two influential, statistically significant predictors are the GDP annual growth rate and the competitiveness index that help to decrease the inflation/vaccination% ratio.
The odds ratio estimates measure the association of variables. The odds ratio is the multiplicative change in the odds for one unit change in regressors. It reveals that an increase in the sales tax rate, unemployment rate, and consumer price index increases the log odds of having a greater inflation/vaccination%, while an increase in the GDP growth rate, competitiveness index, and government debt to GDP decreases this ratio. The results show that the unemployment rate and consumer price index are not statistically significant at 5%.
COUNTRY RANKINGS AND EFFICIENCY SCORES
After identifying the most important factors that contribute to the development of the inflation/vaccination% indicator, health authorities may wish to rank countries according to their performance. However, establishing a comprehensive ranking is not always possible due to various statistical and subjective issues.
Figure 2 demonstrates the inflation-vaccination ratio in relation to the competitiveness index of all countries. This figure shows that African countries generally experience higher inflation and lower vaccination rates, as well as a lower competitiveness index in comparison with other countries.

Figure 2: Inflation/vaccine ratio with respect to the competitiveness index of countries.
The smaller circles indicate a lower inflation/vaccination percentage, while the darker green colour
represents a higher competitiveness index among countries.
Inf-vac: inflation/vaccine.
A more objective method known as DEA has been proposed for measuring a country’s efficiency in fighting against the COVID-19 pandemic.50 This allows authorities to compare a country’s performance with its peers, and a health official can use the DEA’s efficiency ranking system to compare countries and assess potential improvements.
To minimise scaling problems with DEA, the data were converted to standard scores by subtracting each data point from its mean and dividing by the standard deviation of each variable to avoid negative signs in DEA. Then, a constant number equal to the maximum standard score of each variable was added to the converted standard scores of all observations, resulting in positive values (adding a constant number does not change the relative rankings of the observations).
The selection of appropriate inputs and outputs for the DEA was carried out according to the following considerations. To minimise efficiency discrimination power, the number of inputs and outputs was kept to a minimum.50 Moreover, the most relevant input and output variables were used to maximise efficiency of the operations.50 In order to improve efficiency of the operations and facilitate country comparability, the most important explanatory variables were considered. The inflation/vaccine ratio was chosen as the output for the model; consequently, the input variables of GDP annual growth rate and competitiveness index were selected based on logit regression for the DEA model. As the focus of the analysis is on inflation/vaccine ratio, a constant return to scale two-stage output-oriented DEA model was developed based on the identified input and output variables.
The DEA model can be used in various ways, with one of its primary functions being to provide a view of how countries utilise their resources to combat the COVID-19 pandemic. Although wealthy nations generally have higher efficiency, some are still predicted to perform poorly. Table 3 displays the results, which suggest that some of these countries are surprisingly underperforming.
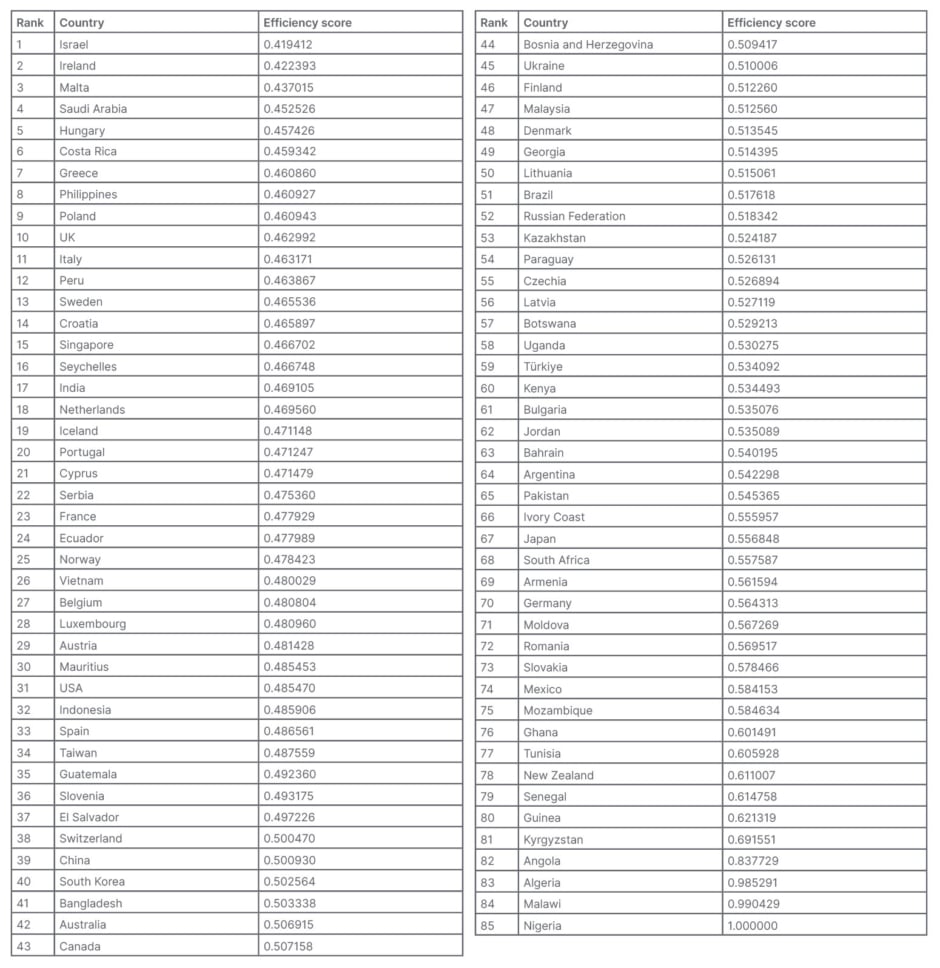
Table 3: Ranking and efficiency scores of countries based on the inflation/vaccination ratio.
*Significant at p<0.05.
†Significant at p<0.10.
Sample size is 85. Government debt to GDP-S is the square of variable Government debt to GDP, and competitiveness index-SR is the square root of the variable competitiveness index.
GDP: gross domestic product; GDP-S: square of the government debt to gross domestic product; SR: square root.
Table 3 shows the DEA efficiency and ranking of the standardised scores of the inflation/vaccine ratio for each country. A larger positive number implies a worse index for the inflation/vaccination ratio. This transformation changed the direction of the inflation/vaccination% rates from minimum to maximum outputs, which is consistent with the DEA directive. For example, Nigeria has an index of 1.00 whereas Israel has an index of 0.42. It can be observed that other African countries, such as Malawi, Algeria, and Angola, have high scores, followed by Ireland, Malta, Saudi Arabia, and then Israel. Nations may be able to follow the health and economic plans of Israel, which would increase productivity levels in their countries. It is noteworthy that there is a minimal difference between the efficiency score of Israel (0.419412, the first rank country) and the score of the USA (0.485470, the 31st rank country). Nearly half of the countries have an efficiency score lower than 0.5, and only the aforementioned African countries have a score greater than 0.7, indicating that the people of these African countries are suffering from the COVID-19 pandemic and require special attention from authorities.
DISCUSSION AND LIMITATIONS
To create a robust model that can better capture the relationship between the vaccination rate and the inflation rate of countries, a binary variable inflation/vaccination% representing the combined effect of vaccine and inflation rates was created. One important reason to examine this binary relationship is that it avoids the assumption that is required for linear regression and allows the examination of nonlinear relationships. The logistic model also allowed for the testing of the interrelationship between vaccination and inflation rates with a group of macroeconomic factors.
The findings show that the pseudo-R2 of logistic regression after including all variables is 89.67%. In the logistic model, annual GDP growth rate and competitiveness index are the most influential factors contributing to the inflation/vaccination% ratio for all countries during the COVID-19 pandemic. (Note: the sales tax rate is also playing an important role in this model, but the authors do not recommend this variable, since reducing the sales tax rate is inversely related to the competitiveness index, and a nation cannot stop using tax funds to build roads or bridges).
These results imply that a country with a higher rate of GDP growth and competitiveness index or lower sales tax rate during the COVID-19 pandemic has a lower inflation/vaccination% ratio. This fraction becomes smaller with a lower inflation rate, a higher vaccination rate, or for both reasons. Another influential macroeconomic factor in this study contributing to the inflation/vaccination% ratio is government debt to GDP. This macroeconomic factor shows the vital role of governmental help (e.g., stimulus checks) in mediating the effect of COVID-19 in a nation.
After finding the most influential variables in explaining the inflation/vaccination% ratio, a constant return to scale constant return to scale two-stage output-oriented DEA model based on the assurance region was used to help the authorities and healthcare systems to better understand the health economic situations of nations worldwide. The DEA inputs and outputs were chosen based on the most significant factors from the above statistics and data elements. The output includes the percentage of a nation’s inflation/vaccination rate, and inputs include the nation’s annual GDP growth rate and competitiveness index. The DEA’s complete dataset was then converted to an easily interpreted format to ensure that the result of the fight against the COVID-19 pandemic is not affected by the few inputs and outputs participating in optimal solutions.
These relationships show it is expected that a nation with a higher vaccination rate has a higher GDP growth rate because people can return to stable work situations,51 businesses are open, and people have improved mental health.52 Open businesses result in increased mobility,53 social capital,54 and global research and development,55 which consequently results in higher production rates. Additionally, avoiding support options such as stimulus checks removes disposable personal income, which feeds inflation for a post-pandemic situation.39-41 Reopening all businesses and getting back to a pre-pandemic economy helps to balance demand and supply, where imbalances are likely to increase inflation.6-8,31
This study has some limitations. For example, a significant change in the consumption baskets of households during the pandemic may disrupt the supply and demand balance in the short and medium terms. Such an imbalance contributes to an overall inflation rate where supply shortages during the lockdown period can result in excess demand due to the reopening and recovery of the economy. In fact, the household baskets change slowly year over year, but the lockdown and remote delivery of jobs created a sudden change in the consumption basket of households, and this abrupt shift affects the equilibrium point of demand and supply in the market; therefore, including other health and economic factors might have the potential to change the results. However, this study’s policy recommendations can aid planners and authorities in creating long-term plans because the findings present strong evidence that countries should regulate vaccination programmes to counteract global inflation during pandemics.
CONCLUSIONS
This study shows that there is an interrelationship between the healthcare variable, vaccination rate, and the economic variable, inflation, during the COVID-19 pandemic worldwide. The findings indicate that inflation and vaccination rates are closely connected and related to each other through other macroeconomic factors. These findings are consistent with the lack of necessity for governments to provide external financial support (e.g., stimulus checks in the USA). An increase in disposable income increases the amount of cash flow in society and therefore leads to an increase in the inflation rate. Additionally, the lack of external support puts additional pressure on individuals to return to work, resulting in a job market boom due to higher GDP growth rate and competitiveness index that controls the inflation rate. The results from this study have the potential to provide invaluable insights to governments, healthcare systems, and policymakers in understanding the economic and health situations of countries and helping them make informed decisions in their fight against the COVID-19 pandemic.






