Author: Sabrina Shah-Desai,1 Billur Sezgin,2 Benji Dhillon,3 Lee Walker,4 Raymond Wu,5 Patrick Trevidic6
1. Perfect Eyes Ltd., London, UK
2. Department of Plastic, Reconstructive and Aesthetic Surgery, Koç University School of Medicine, Istanbul, Türkiye
3. Define Clinic, Beaconsfield and London, UK
4. BCity Clinics, Liverpool, UK
5. Asia Pacific Aesthetic Academy, Hong Kong, China
6. Expert 2 Expert, Paris, France
Disclosure: All speakers have served as consultants for Teoxane.
Acknowledgements: Medical writing assistance was provided by Bárbara Magalhães, Clinical & Medical Affairs Department, Teoxane, Geneva, Switzerland.
Support: The symposium and publication of this article were funded by Teoxane.
Keywords: Aesthetics, dermal filler, hyaluronic acid (HA), psychosocial wellbeing, quality of life.
Citation: EMJ. 2023;8[2]:10-18. DOI/10.33590/emj/10306368. https://doi.org/10.33590/emj/10306368.
Meeting Summary
Perception of beauty is changing from a rigid concept (i.e., the universal idea of beauty) to a multifaceted and personalised view of one’s appearance. One of the main concerns of patients is looking artificial and losing their unique facial expressions, which encourages them to seek aesthetic procedures that yield the most natural results. Patients also wish to increase their self-esteem and, ultimately, improve their quality of life. It is now well-established that treatment with hyaluronic acid (HA)-based dermal fillers improves the psychosocial state of patients. The assessment of facial anatomy and patient needs, accompanied by the proven holistic benefit and good safety profile of HA dermal filler treatment, is also a key factor for an optimal outcome. In addition, clear communication between patient and physician is crucial to manage patient expectations, maximise satisfaction, and minimise procedural risks. The availability of a wide range of HA dermal fillers, customised for specific anatomical areas and facial movements, allows physicians to develop patient-specific treatment plans.
This review of the ‘Elevating Aesthetics’ symposium held at the International Master Course on Aging Science (IMCAS) 2023 shares insights into the patient’s facial anatomy and possible danger zones presented during a cadaver workshop. Several successful treatment plans tailored to different patient profiles (i.e., patients seeking full-face aesthetic improvement, patients with facial asymmetry, low lip volume in mature and millennial women) were also implemented live. A comprehensive and patient-specific HA dermal filling treatment should be considered by physicians to achieve natural outcomes and improve the general wellbeing of the patient.
Part 1: Impact of Hyaluronic Acid Dermal Fillers on Psychosocial Wellbeing
Sabrina Shah-Desai
During the ‘Elevating Aesthetics’ symposium, held at IMCAS 2023 and moderated by Patrick Trevidic, Expert 2 Expert, Paris, France, Sabrina Shah-Desai, Perfect Eyes Ltd., London, UK, presented the concept of individual beauty and how aesthetic treatments are not only about vanity, but also about improving the general wellbeing of the patient.
The ideal of classical beauty is changing. In Ancient Greece, beauty was defined in terms of harmonious proportion of facial features, and the ‘perfect’ human face was based on Plato’s system of triads.1 Although the Greek definition is still seen as the standard, the popularity of this prototype is influenced by social trends and historical events.2 In fact, the notion of facial beauty is expanding nowadays into many different disciplines, such as psychology, evolutionary biology, sociology, cognitive science, and neuroscience.3-7 It has been demonstrated that cultural intra- and interpersonal differences influence attractiveness perception in different ways,7 which renders the concept of beauty more complex, but also more fluid and subject-specific.
The gradual shift to an ‘individual beauty’ concept is accompanied by the current trend of subtle enhancement in facial aesthetics, with an emphasis on natural-looking outcomes, maintenance of unique facial expressions, and popularisation of minimally invasive techniques.8 Soft-tissue fillers are the second most preferred minimally invasive treatment and HA products are currently the most used soft tissue fillers.9 The availability of a wide range of HA dermal fillers customised for specific anatomical areas with different facial movements allows physicians to elevate their treatment plans to achieve natural facial dynamism.10-12 Panels of experts have defined key strategies to achieve natural-looking results when injecting HA fillers: patient assessment and individualisation of treatment plan, adequate knowledge of facial anatomy, proper injection techniques, good knowledge of the rheological properties and behaviours of different HA fillers, and a conservative treatment approach.13,14
Patients are not only looking to improve their appearance, but also their mental and emotional health, along with social wellbeing.15 In a survey on patient motivations to undergo cosmetic procedures, psychosocial concerns were mentioned more than other identified themes, specifically the appeal for improved confidence, feeling depressed and anxious with current appearance, and feeling consumed by efforts to conceal undesirable physical features.16 Other studies have demonstrated significant psychological and social benefits from HA filler treatment, in addition to considerable improvements in self-perceived appearance and age.15,17 These results confirm that benefits from HA filler injections extend beyond mere physical improvements.17
Part 2: Live Demonstration– Patient Empowerment After Full-Face Injection
Billur Sezgin and Benji Dhillon
From a practitioner’s perspective, it is essential to clearly explain the treatment plan to the patient and reach an agreement between the physician and the patient to manage the latter’s expectations, maximise satisfaction, minimise procedural risks, yield the best aesthetic outcomes, and, ultimately, improve the patient’s quality of life.
Full-Face Anatomy and Danger Zones
Proper knowledge and understanding of the facial anatomy and danger zones can mitigate risks during dermal filler injections, as well as potentiate natural-looking results. Billur Sezgin, Department of Plastic, Reconstructive and Aesthetic Surgery, Koç University School of Medicine, Istanbul, Türkiye, conducted a human cadaveric dissection to outline the multi-layered facial anatomy and summarise danger zones to avoid when injecting each facial region.
Sezgin displayed the facial arrangement in several layers that can be described from superficial to deep: layer 1, skin; layer 2, subcutaneous fat; layer 3, superficial musculoaponeurotic system; layer 4, deep fat; and layer 5, bone.18 However, this general distribution needs to be adapted to each facial region, as there are regions composed of more (e.g., temple with 10 layers) or fewer layers (e.g., tear through with three layers).18
The subcutaneous fat layer extends throughout the facial surface, and its thickness and presence varies across facial region. As treatment with dermal fillers increases volume of tissue, knowledge on regional thickness and distribution of the facial superficial fat is essential to determine injection depth and layer.19 Layer 2 is segmented by fibrous septae into different compartments, which serve as sheltered transit pathways for cutaneous nerves and vessels.20 The superficial musculoaponeurotic system layer separates the superficial and the deep fat, and creates facial expression through transmission of the muscles’ contraction to the skin.21,22 The dynamism of the connection between superficial fat pads and the underlaying muscle plane should be well understood to avoid appearance of lumps upon muscle contraction.22 The deep fat is also divided into distinct compartments, and their outline serves as conduits for facial nerve branches and for the branches of the facial artery and vein.20 The facial skeleton support diminishes with age as the bones recede and remodel, which leads to the inferior and medial repositioning of fat pads and muscles over the bony foundation.23,24 As deep fat compartments seem to be relatively stable during ageing, deep filler injection in this layer and in contact with the bone provides support for the overlying structures, and increases projection.25
Extensive knowledge of the location and pathway of facial blood vessels in the upper, middle, and lower face is essential to minimise the risk of complications associated with vascular injuries. Sezgin continued the cadaver dissection by reminding the audience about the facial vascular anatomy.14,26-29 Three branches of the external carotid artery provide blood supply of the facial skin: the facial artery, superficial temporal artery, and transverse facial artery, which is a branch of the superficial temporal artery.26 Over the neck, at the premasseter ligament region, two vascular structures enter the face: the facial artery and the facial vein. One of the facial artery branches, the submandibular artery, is located underneath the mandibular border. Another branch, approximately 6 mm lateral to the midline of the chin, is the submental artery. Following the course of the main artery, the inferior labial artery is found underneath the depressor anguli oris and enters the lower lip. The facial artery continues to follow its oblique tortuous course and reaches below the zygomaticus major muscle, accompanying the nasolabial fold, where it branches into the superior labial artery at the upper lip. After arriving at the nasal base, the facial artery continues superficially along the lateral wall of the nose and ends as the angular artery. It shares multiple connections and anastomoses with the internal carotid system, as well as with the supratrochlear and supraorbital artery. The transverse facial artery is close to the parotid duct, and the superficial temporal artery is found within the superficial temporal fascia. The latter supplies the forehead, the lateral portion, and the temple region. An additional branch, the infraorbital artery, is observed middle to the pupillary line and follows its counterpart nerve.
Sezgin highlighted the importance of mastering the facial anatomy when injecting, not only to avoid vascular compromise, but also to ensure the injection is performed in the desired and correct compartments. Superficial fat compartments that enlarge with age (e.g., nasolabial fat pads, jowl fat) should be avoided. Additionally, the infraorbital superficial fat pads should also be bypassed as this region comprises a very delicate lymphatic system, and its treatment can accentuate palpebromalar bags.
Patient Assessment
Benji Dhillon, Define Clinic, Beaconsfield and London, UK, introduced their 51-year-old female patient who saw their confidence plummet over the years after experiencing several traumatic events. The patient was unhappy with age-related changes that rendered their cheeks more prominent and gave them harsh facial features. They were also self-conscious about their lips, which impacted their behaviour during social interactions. Tooth loss on the right side of the face further contributed to the increased concavity in their mid- to lower cheek and to the asymmetry between both sides of the face. Female patients tend to experience a decreased chin projection as they get older, since their mandibles rotate inferiorly and backwards toward the skull.18,19 This age-related transition further accentuated the patient’s retrognathic chin and overbite. By undergoing HA dermal filler treatment, the patient wished to feel more confident, stronger, and empowered.
Patient-Specific Full-Face Treatment
Temple
Dhillon injected the highly spreadable Teosyal RHA 1 (Teoxane, Geneva, Switzerland) at the temple region, into the inter-fascial plane. A product with high stretch was used since the deficiency of volume in this area was non-significant, and the treatment objective was only to improve the transition from the forehead towards the temple.30,31 As the superficial temporal artery accompanies the hairline, a more posterior deposit of filler should be avoided. To treat the roof of the brow, Dhillon adjusted the depth of the cannula towards the deep fat compartment and injected small amounts of product moving towards the lateral canthus, at the lateral orbital rim, while avoiding the infraorbital superficial fat compartment. Treatment details are described in Figure 1.
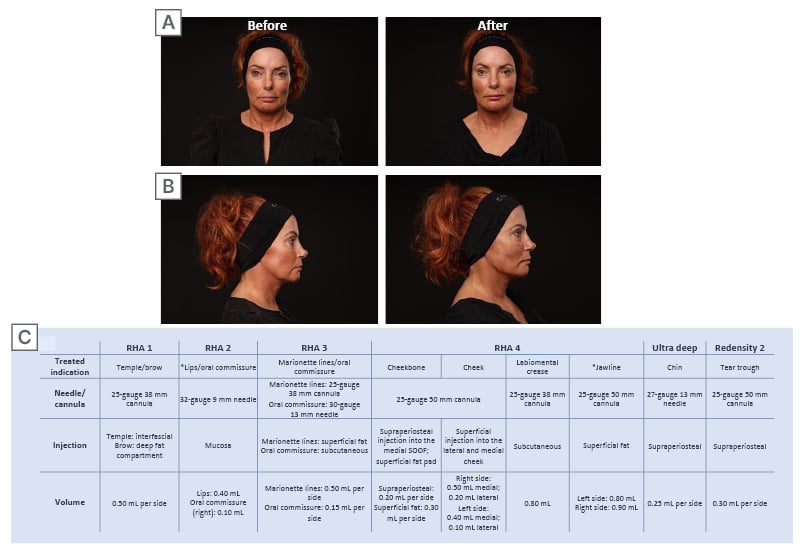
Figure 1: Full-face treatment of a mature female patient with low self-confidence.
A) Front facing and B) profile before and after photographs of a mature female patient with low self-confidence, who received full-face treatment with TEOSYAL (Teoxane, Geneva, Switzerland) fillers. C) Treatment summary.
*Lip and jawline treatment was not demonstrated live.
Midface
Teosyal RHA 4 (Teoxane) was chosen for the cheekbone injection, a versatile volumiser with very high strength and good stretch, since the patient did not require a large volumisation in this region (Figure 1).30,32 A small bolus was injected supraperiosteally with a cannula in the medial suborbicularis oculi fat compartment, entering from the zygoma. The same entry point was used to treat the superficial fat pad where a long thread of filler was injected, retrograding towards the entry point. At this stage, the patient showed inexistence of lumps and bumps, as well as animation deformities. Dhillon reminded the audience to avoid the infraorbital fat compartment when injecting this region as it has a rich lymphatic plexus, and also enlarges with time.
Tear trough
The tear trough was treated with Teosyal PureSense Redensity 2 (Teoxane; Figure 1). Its low hygroscopy and high spreadability are adapted for the correction of under-eye circles.33,34 Using the same entry point as for the cheekbones, micro threads of product were injected supraperiosteally with a cannula while performing a fanning technique.
Mid- to lower face
Treatment of the inferior portion of the middle and lateral cheek fat compartment is normally avoided due to its closeness to the nasolabial and jowl fat compartments. However, treating this region could improve the patient’s hollowing caused by missing teeth. Teosyal RHA 4 was injected with a cannula towards the medial cheek, at a superficial plane (Figure 1). Threads of product were deposited retrogradely to restore the transition to the lower face and soften patient features. A posterior tunnel from the previous entry point was created to minimise pain and bruising during the posterior injection. After treating the lateral fat compartments, threads of product were injected above the zygomatic arch to improve the mid-cheek to lower face transition.
Chin
The pogonion was treated with the highly cohesive and resistant to compression Teosyal PureSense Ultra Deep (Teoxane [Teoxane, unpublished data]; Figure 1), which is designed to provide deep structural support and maximum lifting capacity.34 It was injected supraperiosteally with a needle to attenuate the patient’s retrognathic chin and improve their facial profile.
Labiomental crease
Teosyal RHA 4 was injected with a cannula into the subcutaneous plane using a micro-fanning technique to decrease the shadowing observed in their lower face. Dhillon reinforced the flexible strategy of assessing the aimed outcome and adapting the treatment during injection, instead of rigorously following the planned injection volumes.
Marionette line and oral commissure
A strong and highly stretchy product (Teosyal RHA 3 [Teoxane]) was used to guarantee the dynamic volumisation of the marionette lines.30,35 The techniques applied to treat this region should respect the correct placement of the filler to avoid weighing down a superficial fat compartment. Treatment injection was performed medial to the mandibular ligament, progressing up towards the oral commissure, and depositing long and short threads of product retrogradely with a cannula. Dhillon superficially injected a small bolus of Teosyal RHA 3 in the oral commissure using a needle. Lastly, they injected the inferior vermillion border close to the oral commissure, acknowledging the position of the inferior labial artery, which enters the lip medial to the injection site.
Before and after photos can be seen in Figure 1, with visible improvement of the anterior midface projection, decreased infraorbital hollowing, and improvement of their middle to lower face transition and profile.
Patient satisfaction after 1 month of treatment
The patient was requested to answer a short survey 1 month after treatment, which combined questions on injection experience, impact of HA fillers on quality of life, and overall treatment satisfaction. They experienced no pain during injection. Although their improvement in self-esteem has been gradual, they felt more comfortable during social interactions, and more inclined to look at their own reflection. They also declared feeling more confident, beautiful, and empowered while still looking like themself and maintaining their defining facial features.
Part 3: Patient-Tailored Lip Treatment
Lee Walker
Lee Walker, BCity Clinics, Liverpool, UK, kickstarted this session by accentuating how lip treatments can visually impact facial aesthetics. The lips are an essential component of the symmetry and aesthetics of the face,36 with full lips being historically associated with female youth, beauty, and voluptuousness.37 The perioral tissues increasingly deteriorate with age.38 Prominent signs of labial ageing include the lengthening of the cutaneous upper lip, development of rhytids, collapse of the oral commissures, inversion of the red vermillion, drooping mouth corners, and flattening of cupid’s bow and philtrum columns.39
Lip augmentation procedures are increasingly popular, with nearly 2.6 million injections (e.g., soft tissue fillers) performed in 2018, and a total increase of 312% between 2000 and 2017.9 According to Walker’s clinical experience, lip treatments are even the most requested dermal filler procedures. Once again, most of the patients (73%) requesting dermal fillers wish to achieve natural and healthy-looking lips. Nonetheless, a natural look requires a thorough knowledge of the perioral anatomy, the range of products that better suit this region, and technique.37 The main goal when treating this area is to create a shape that aesthetically harmonises with the patient’s unique facial features, and considers their age and ethnic background.37
Live Demonstration: Patient Self-Confidence After Lip Treatment
Raymond Wu and Patrick Trevidic
Mature lip
Raymond Wu, Asia Pacific Aesthetic Academy, Hong Kong, China, continued the session by treating a 59-year-old female patient with age-related loss of lip volume. The patient acknowledged an offset between their sportive physique and their thin lips, which made them look older than they felt. They wished to improve the appearance of their smile and lips and regain their self-confidence.
Assessment of the patient anatomy revealed an obvious depletion of the upper and lower lip volume, as well as downturned mouth corners. They lost all their upper teeth and wore a dental prosthetic. Shortening of the lower third of the face, deeper wrinkles, and prolapse of the labial commissure are examples of facial soft tissue collapse in subjects with edentulism.40 Wu emphasised the importance of assessing the perioral area in a mature lip, such as the existence of barcode lines.
Wu started the treatment with an HA filler (TEOSYAL RHA 3) combining high strength and good stretch, which ensures dynamic lip volumisation. With a cannula, they entered the corner of the oral commissure and injected the subcutaneous plane of the lip with small droplets of product to anaesthetise the region. Afterwards, the treatment injection was performed very slowly but dynamically (i.e., back and forth movements) to avoid any vascular compromise.
To provide more definition to the vermillion border and cupid’s bow, Wu used a needle to inject superficially and retrogradely the vermillion border from the corner of the mouth, at two different entry points. Subsequently, they treated the cupid’s bow by applying a mini fanning technique at the midline to achieve more natural results in the upper lip. The product of choice was an HA dermal filler with high stretch and moderate strength (TEOSYAL RHA 2 [Teoxane]), which allows dynamic lip reshaping.30,41 Lastly, two boluses were injected in the vermillion border, at each side of the lower lip, to improve contouring.
A product with very high stretch (TEOSYAL RHA 1) that adapts uniformly to superficial dynamic wrinkles was applied to the perioral lines. Small boluses of product were placed laterally and intradermally with a needle to improve barcode lines, but also the skin quality of this region.
Wu manoeuvred through a wide range of products that can be used in several indications of the perioral region. The treatment yielded a visible improvement of perioral rhytids, lip volume, and contour, while retaining an age-appropriate outcome (Figure 2).
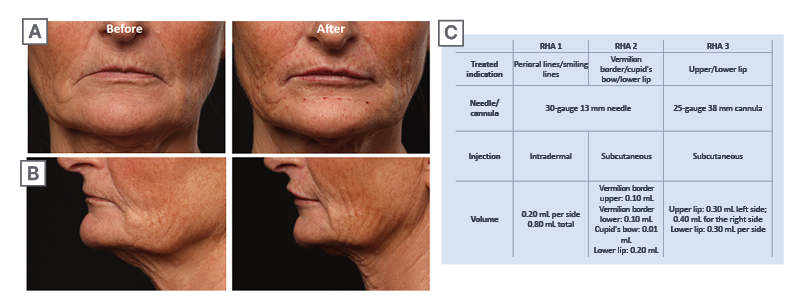
Figure 2: Lip treatment of a mature female patient.
A) Front facing and B) profile before and after photographs of a mature female patient who received lip treatment with TEOSYAL (Teoxane, Geneva, Switzerland) fillers. C) Treatment summary.
One month after treatment, the patient described no pain during injection and no evident bruising or swelling. The treatment was unnoticed by their acquaintances, which supports the natural outcome of HA filler treatment. Dermal filler injections improved their appearance, boosted their self-confidence, and led them to elevate their posture during social interactions. Overall, this procedure evidently improved the patient’s quality of life.
Millennial lip
Trevidic introduced a 23-year-old female patient who demonstrated volume imbalance between the upper and lower lip, with the upper lip being much thinner than its counterpart. They have been mocked because of the lack of upper lip volume, which took a toll on their self-esteem. For this patient, conservative dermal filler treatment could change the way others perceive their appearance and, most importantly, it could boost their self-confidence and complement their already radiant personality.
In conjunction with the low upper lip volume, Trevidic identified an asymmetry between the left side and the right side of the upper lip, with the latter showing less volume. As the cupid’s bow and the vermillion border were well defined in this patient, Trevidic reinforced two important points to be considered when defining this patient’s treatment plan: maintain the balance of the upper and lower lip and avoid over-volumising the lips. Treatment details are described in Figure 3.
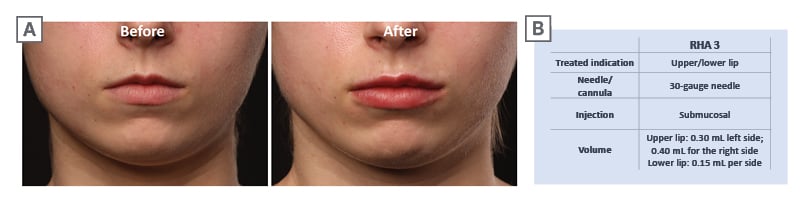
Figure 3: Lip treatment of a millennial female patient.
A) Before and after photographs of a millennial female patient who received lip treatment with TEOSYAL (Teoxane, Geneva, Switzerland) fillers. B) Treatment summary.
The injection was performed with the dynamic filler TEOSYAL RHA 3. Entering the cupid’s bow in the vermillion border, small amounts of product were injected slowly with a needle in the mucosa to allow the lidocaine to anaesthetise the region before volumisation injection. Trevidic emphasised the dangers of injecting the submucosa. Injections should be less than 3 mm deep, with an intermediate or low-G filler, at the vermillion cutaneous border or within the red dry vermillion.42 Using the same anaesthesia entry point, Trevidic injected the submucosa horizontally and in a retrograde manner. They then used a second entry point oblique to the first to further volumise the lips.
With conservative amounts of product, the patient’s lips were volumised to a natural-looking degree and the asymmetry between the right and left upper lip was corrected (Figure 3).
On their 1-month post-congress testimonial, the patient described having barely any bruising and that the swelling disappeared after a couple of days. The treatment outcome was natural and aesthetically pleasing, while maintaining lip mobility and facial expressions. It also enabled them to behave comfortably and confidently during social interactions. The patient was fulfilled with the treatment plan adapted to their concerns and expectations, and would recommend it to anyone with self-confidence issues.
Conclusion
Beauty perception is evolving from an ancient, rigid, and ‘universal’ perspective to a multidisciplinary and individualised concept. No matter the indication, patients seek subtle facial enhancement procedures that yield natural-looking outcomes in harmony with their unique facial expressions but, most importantly, treatments that will ultimately improve their psychosocial well-being. Extensive evidence has demonstrated the positive impact of HA dermal fillers on the patient’s quality of life. The holistic benefit and safety of these products, coupled with comprehensive and patient-specific treatment plans, should be considered by physicians to achieve natural outcomes, and improve the general wellbeing of the patient.





