
BACKGROUND
The latest American Heart Association (AHA)/American College of Cardiology (ACC) cholesterol guidelines on primary prevention of coronary artery disease recommend the use of the absolute coronary artery calcium (CAC)-score to help decision making for using statins. If the CAC-score is 0, it is reasonable to withhold statin therapy if more severe conditions are absent. If the CAC-score is 1–99, it is reasonable to initiate statin therapy for patients ≥55 years of age. If the CAC-score is ≥100, initiation of statin therapy is recommended. In this present analysis, the authors assessed the impact of these guidelines in everyday cardiology practice.
PATIENTS AND LIMITATIONS
- 16,083 people (males: 11,271; females: 4,812).
- If individuals had several CT scans, only the first scan was included.
- Data were prospectively collected in a dedicated data base (FileMaker Pro [Claris International Inc., Santa Clara, California, USA]).
- Only people for primary prevention were analysed.
- Patients had no or very atypical chest pain.
- Patients with exercise-dependent chest pain or shortness of breath were excluded.
- Individuals with cardiac catheterisation were excluded.
- Limitations included: lack of calculation of the many recommended risk scores for atherosclerotic cardiovascular disease, there was no data on low-density lipoprotein cholesterol, and patients with diabetes were included.
RESULTS
In the middle-age group, approximately one-third of males and two-thirds of females would not need a statin, whereas one-third of males and 10% of females would need a statin. Thus, the coronary calcium score has shown it could be valuable in individualised medicine. Please see Table 1.
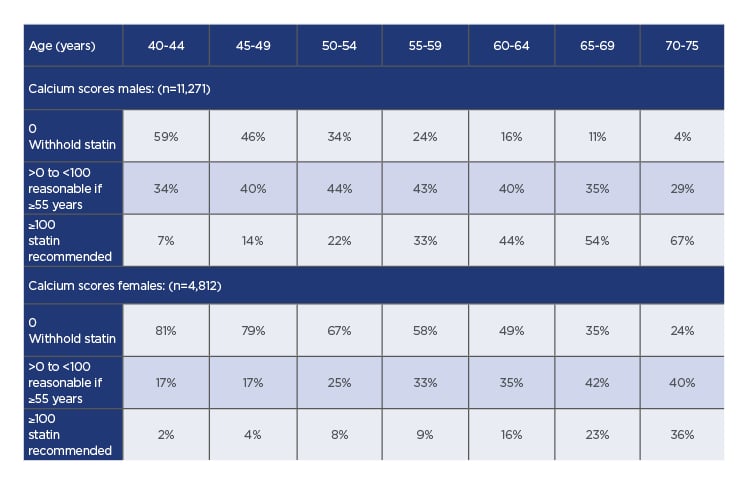
Table 1: Calcium scores according to sex and age groups.
SUMMARY AND CONCLUSIONS
1. In patients between 40 and 75 years of age, without diabetes, low-density lipoprotein cholesterol <190 mg/dL (<4.9 mmol/L), and a 10-year risk in the middle range (5.0–19.9%), the use of statins is uncertain.
2 The decision for statins should be taken very seriously because it is for life and comprises side effects.
3. The only ‘risk enhancer’ with a practical instruction for decision making in individual cases is the CAC-score. This recommendation is based on the absolute value of the calcium score.
4. This new form of recommendation makes the interpretation of the calcium score faster, easier, and more reliable than it is according to percentile distribution.
5. Considering the limitations mentioned for this analysis, in the authors’ cardiology practice the use of calcium score in ‘middle-aged persons’:
– Could avoid statin prescription in approximately 30% of male and approximately 60% of females.
– On the other hand, the use of statins is reasonable in approximately two-thirds of higher aged males and one-third of higher aged females for primary prevention in individuals who otherwise would not receive it.
6. Besides this, the CAC-score enables direct visualisation of the disease and, therefore, increases adherence to the therapy with statins and other cardiovascular drugs.






