
INTRODUCTION
Data are limited on the efficacy of medical therapies for non-syndromic thoracic aortic aneurysms (TAA), with expression of disease-causing genes restricted to vascular smooth muscle cells (VSMC) and disease manifestations restricted to the aorta, in contrast to syndromic TAA, which is associated with abnormalities of multiple organ systems (particularly in Marfan syndrome).1,2 However, accumulating evidence has demonstrated that renin-angiotensin system activity through the VSMC is strongly associated with the formation and progression of TAA.3,4
The aim of this study was to evaluate the effect of angiotensin-converting enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB) therapy on ascending aortic diameter progression in patients with non-syndromic TAA.
METHODS
Fifty consecutive patients (mean age: 57.9±14.9 years) with TAA were enrolled in our retrospective, non-randomised, single centre study after aortic surgery (with or without valve sparring). Preoperatively, in addition to beta-blockers, 17 patients (34%) received ACEI (perindopril, enalapril, or fosinopril), 18 patients (36%) were treated with an ARB regimen (losartan or valsartan), and 15 patients (30%) did not receive any ACEI or ARB medications. Repeated (in 2.39±1.73 years) preoperative CT with three-dimensional reconstruction was used to evaluate aortic diameters and aortic dilatation rate. Left ventricular function and dimensions were examined during preoperative transthoracic echocardiography. Histopathological analysis of resected aortic tissue specimens was conducted after surgery of the ascending aorta.
RESULTS
The mean ascending aortic diameter in the overall group did not change significantly during the preoperative follow-up (from 44.6±7.2 mm to 44.9±6.3 mm; p=0.86). The aortic growth was 0.17±1.33 mm/year in patients receiving ARB but significantly higher, 2.0±0.81 mm/year, in ACEI patients (p=0.04) and 3.0±1.58 mm/year (p=0.01) in patients who did not receive ARB or ACEI therapy.
Global systolic left ventricular function (ejection fraction measured by the Simpson methodology) was slightly depressed in all subgroups: 53.1±10.3% in ACEI, 55.5±10.2% in ARB (ACEI versus ARB; p=0.49), and 58.6±8.0% in control patients (p=0.35 and p=0.10; versus ACEI and ARB, respectively).
No interaction was found between aortic valve morphology and aortic dilatation rate. Bicuspid aortic valve was identified in 18 patients (37.5%), while tricuspid valve interaction was identified in 32 patients (62.5%). Bicuspid aortic valve patients were younger than their tricuspid aortic valve counterparts (47.2±12.2 versus 60.0±10.8 years, respectively; p<0.0001), but aortic root dilatation rate did not vary between bicuspid aortic valve and tricuspid aortic valve patients (1.0±2.9 versus 1.85±1.2 mm/year; p=0.50).
Patients with medial degeneration in tissue samples, including elastic fibre fragmentation, cystic medial change, and smooth muscle cell necrosis (Figure 1), and had lower preoperative ascending aortic dilatation rates compared with patients with histological features of atherosclerosis (0.8±1.03 versus 3.1±2.26 mm/year; p=0.007) in the ARB group.
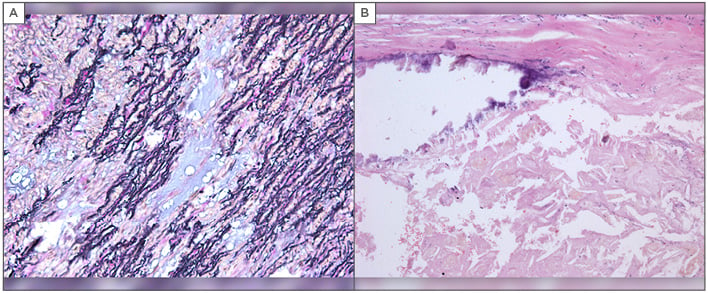
Figure 1: Histologic examination of resected aortic tissue specimens after aortic surgery.
A) Medial degeneration of the thoracic aorta, elastic fibre fragmentation, and cystic medial change; B) An aortic plaque formed through the accumulation of lipids in the intima-media layer of the aorta.
CONCLUSION
Blockade of the renin-angiotensin system pathway by ARB may have a beneficial effect on aortic growth in patients with non-syndromic TAA irrespective of aortic valve morphology. Medial degeneration with smooth muscle cell necrosis, which plays a crucial role in the pathogenesis of ascending TAA, is likely to be the main predictor of the response to ARB therapy.






